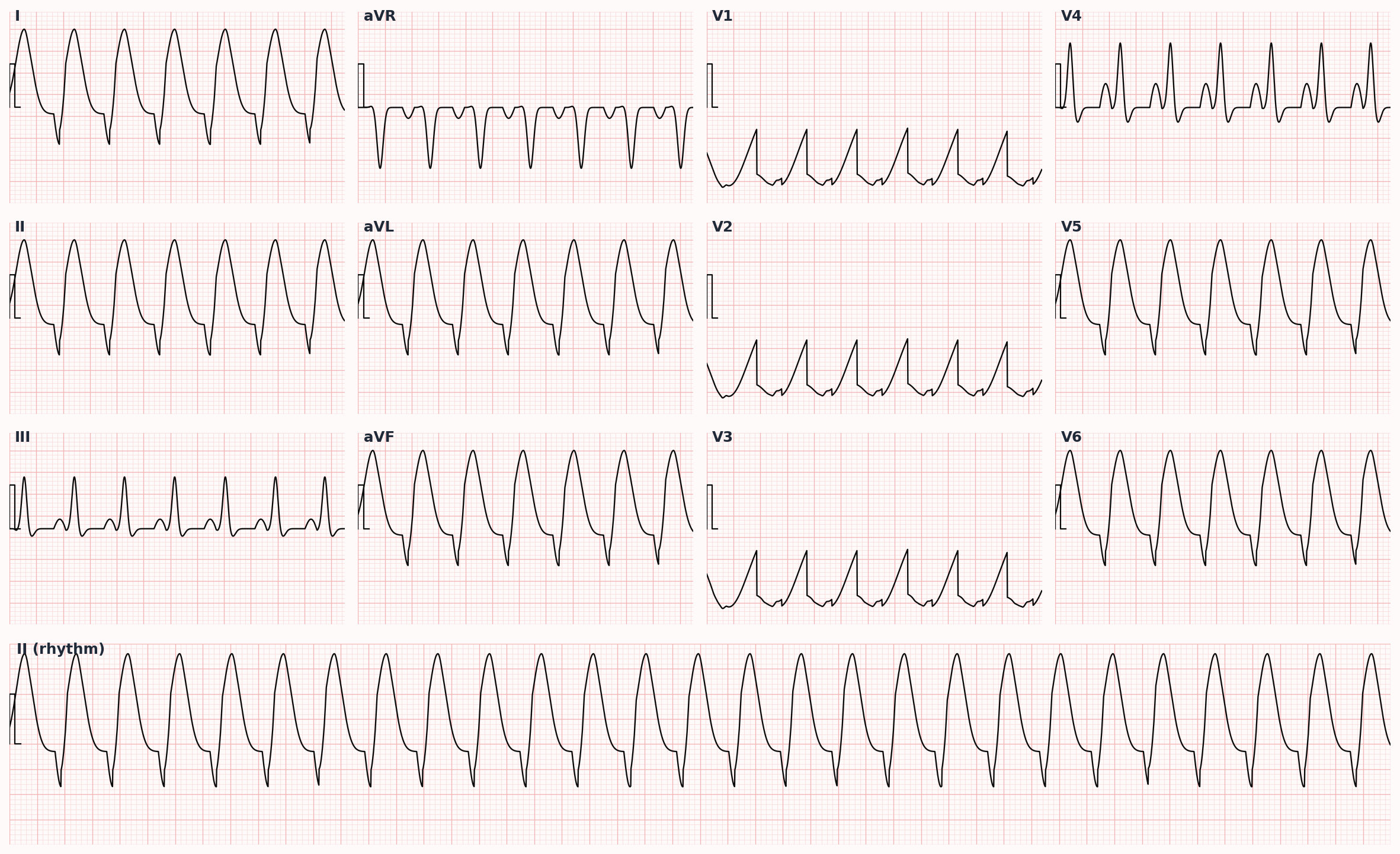
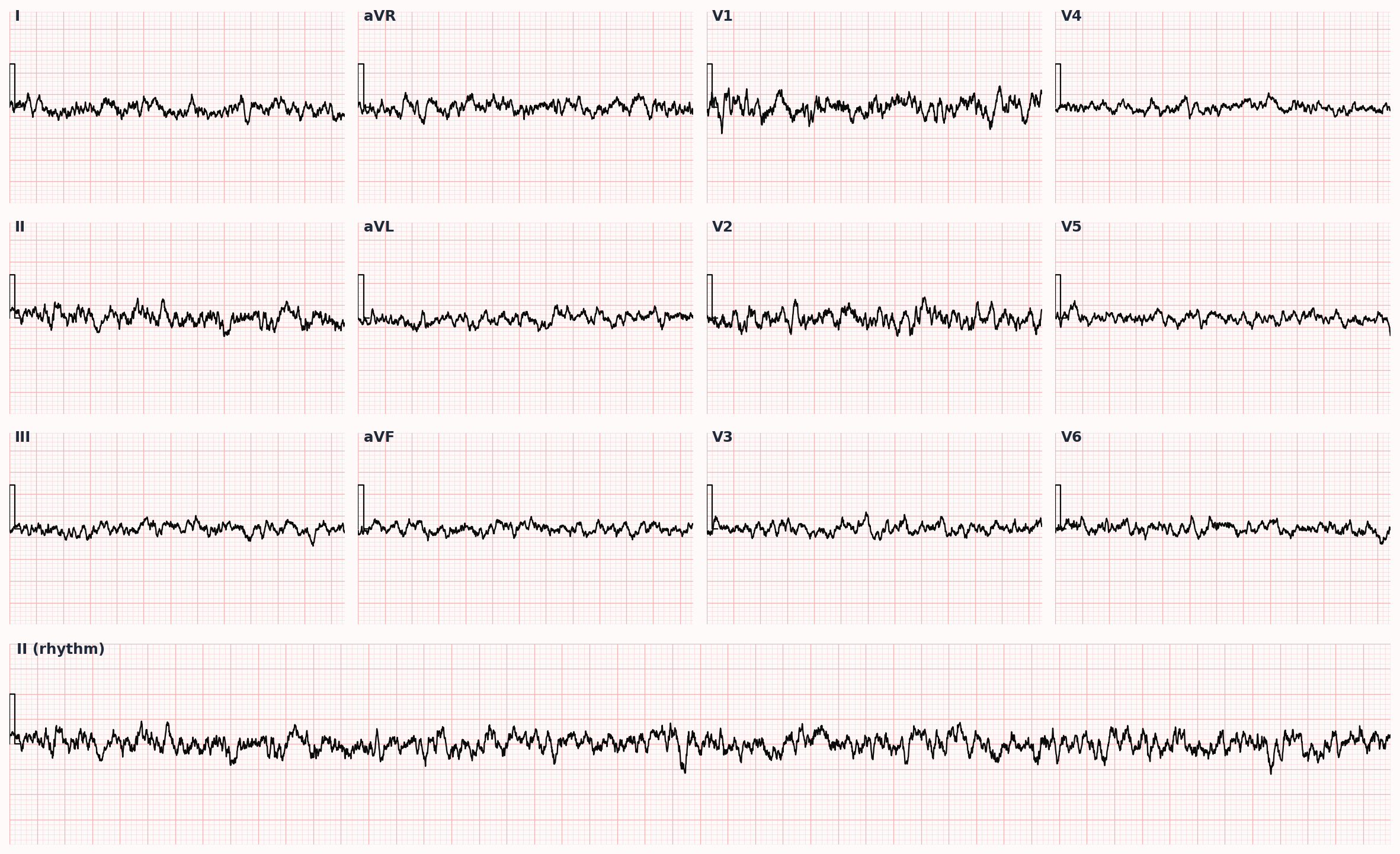
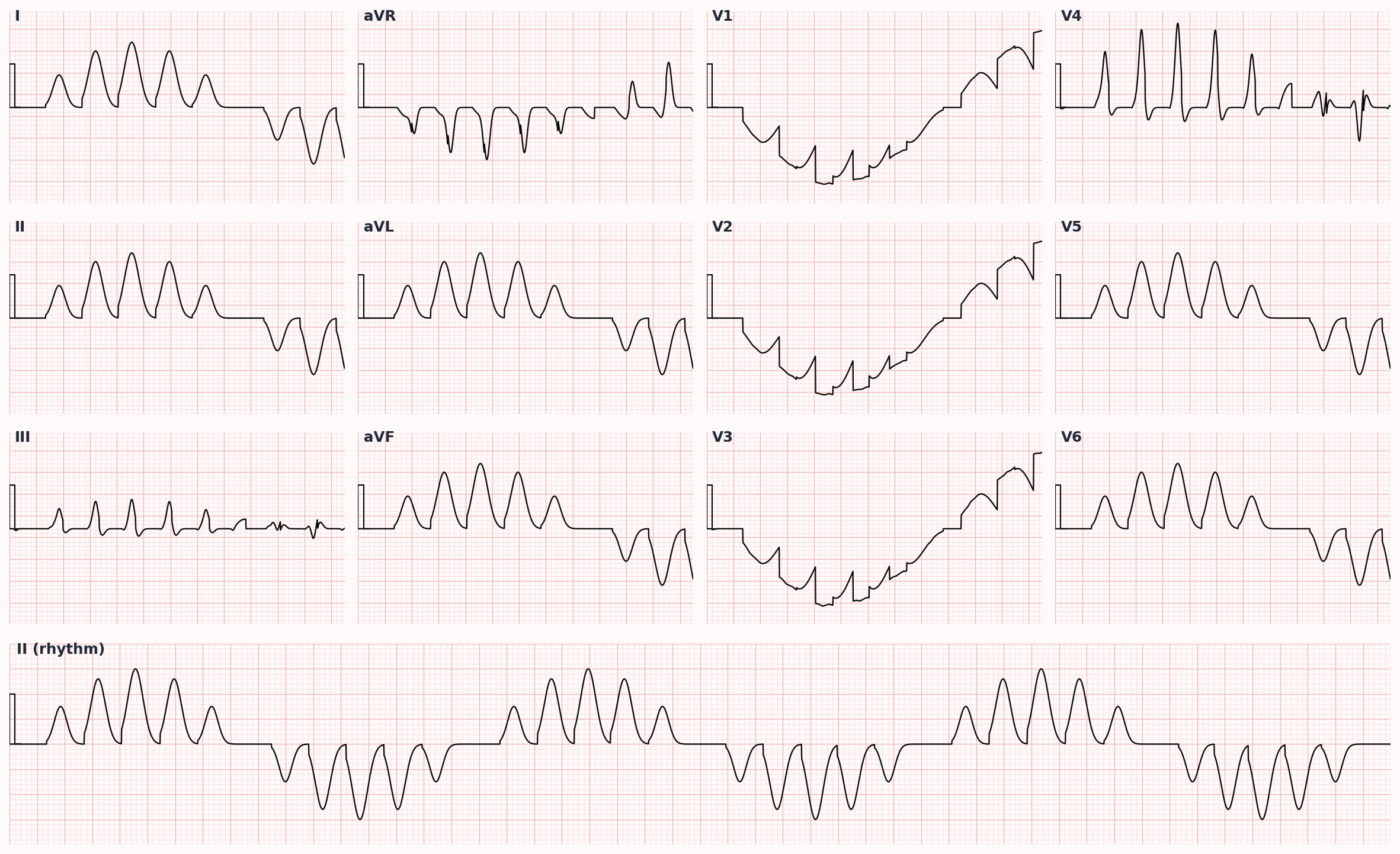
Ventricular Tachycardia and Ventricular Fibrillation
Wide-complex arrhythmia from the ventricle — VF and pulseless VT are cardiac arrest rhythms requiring immediate defibrillation.
Also known as: VT, VF, ventricular tachycardia, ventricular fibrillation, VTach, VFib, wide complex tachycardia
Overview
Ventricular tachycardia is ≥3 consecutive ventricular beats at rate >100 bpm; sustained if >30 s or causes hemodynamic compromise. Ventricular fibrillation is disorganized rapid ventricular electrical activity producing no effective cardiac output.
Epidemiology
Ventricular arrhythmia accounts for the majority of sudden cardiac deaths (~300,000/year US). Most cases occur in patients with structural heart disease, particularly post-MI ischemic cardiomyopathy.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Ventricular Tachycardia and Ventricular Fibrillation outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Coronary artery disease and prior MI (scar-related reentry — most common substrate)
- Heart failure with reduced EF (LVEF ≤35%)
- Hypertrophic, dilated, or arrhythmogenic RV cardiomyopathy
- Inherited channelopathies: long QT, Brugada, catecholaminergic polymorphic VT, short QT
- Electrolyte abnormalities: hypokalemia, hypomagnesemia, hypocalcemia
- QT-prolonging drugs: methadone, ondansetron, fluoroquinolones, macrolides, antipsychotics, antiarrhythmics
- Acute ischemia, myocarditis, cardiac sarcoidosis
- Stimulant use (cocaine, methamphetamine)
Pathophysiology
Most sustained VT in adults is scar-related macroreentry around fibrotic post-infarct tissue. Triggered activity (early or delayed afterdepolarizations) and abnormal automaticity also produce VT, especially in long QT syndromes (torsades de pointes) and in catecholamine-driven states. VF is multiple wandering wavefronts producing chaotic activation and no coordinated contraction.
Clinical presentation
Symptoms
- Palpitations, lightheadedness, syncope
- Chest pain, dyspnea
- Cardiac arrest in VF or pulseless VT
- Some patients tolerate sustained monomorphic VT for minutes-hours with mild symptoms
Signs / physical exam
- Hemodynamic compromise: hypotension, altered mental status, pulmonary edema
- Cannon A waves (AV dissociation in VT)
- Variable S1 intensity (AV dissociation)
- Absent pulse and unresponsiveness in VF / pulseless VT
Differential diagnosis
- Supraventricular tachycardia with aberrancy — Wide QRS from rate-related or pre-existing bundle branch block; Brugada and Vereckei algorithms favor SVT; respond to adenosine
- Antidromic AVRT (WPW) — Wide-complex tachycardia in pre-excited patient; treat with procainamide; AVOID AV nodal blockers
- Pre-excited atrial fibrillation — Irregularly irregular wide complex tachycardia in WPW; can degenerate to VF; treat with procainamide or DC cardioversion
- Hyperkalemia — Sine wave on ECG, peaked T waves, history of CKD, treat with calcium gluconate, insulin/D50, kayexalate
- Pacemaker-mediated tachycardia — Paced device patient with rapid wide complex; magnet application terminates
- Artifact — Patient awake and well-appearing, baseline ECG between artifact, regular underlying rhythm visible
Diagnostic workup
Diagnostic criteria
VT criteria favoring ventricular origin: AV dissociation, capture/fusion beats, QRS >140 ms RBBB or >160 ms LBBB morphology, concordance in precordial leads, extreme axis deviation. When in doubt about wide-complex tachycardia, treat as VT.
Labs
- BMP, magnesium, calcium
- Troponin (ischemia), TSH
- Drug screen if stimulant use suspected
- Digoxin level if applicable
Imaging
- 12-lead ECG during tachycardia and after conversion (look for old MI, QT, Brugada pattern, epsilon waves)
- Echocardiogram — structural disease, EF, scar burden
- Cardiac MRI for scar mapping, sarcoidosis, ARVC
- Coronary angiography to evaluate ischemic substrate
- Electrophysiology study for selected patients and ablation planning
Diagnostic algorithm
flowchart TD
A[Wide-complex tachycardia] --> B{Pulse?}
B -->|No| C[Pulseless VT / VF<br/>Defibrillate 200 J<br/>CPR + epi + amiodarone]
B -->|Yes| D{Hemodynamically<br/>stable?}
D -->|No| E[Synchronized cardioversion<br/>100 J biphasic]
D -->|Yes| F[12-lead ECG<br/>IV antiarrhythmic:<br/>amiodarone or procainamide]
F --> G{Conversion?}
G -->|No| E
G -->|Yes| H[Identify cause<br/>Echo, electrolytes, ischemia]
H --> I{Structural disease?<br/>EF ≤35%?}
I -->|Yes| J[ICD ± ablation]
I -->|No| K[Channelopathy workup<br/>or idiopathic VT ablation]Treatment
First-line
- PULSELESS VT or VF: immediate unsynchronized defibrillation 200 J biphasic, resume CPR, epinephrine 1 mg IV q3-5 min, amiodarone 300 mg IV bolus then 150 mg, treat reversible H's and T's
- UNSTABLE VT with pulse (hypotension, altered mental status, ischemia, pulmonary edema): synchronized cardioversion 100 J biphasic
- STABLE VT with pulse: IV antiarrhythmic — amiodarone 150 mg IV over 10 min, procainamide 20-50 mg/min (preferred for monomorphic VT in many guidelines), or lidocaine 1-1.5 mg/kg IV
- Torsades de pointes: magnesium sulfate 2 g IV, withdraw QT-prolonging drugs, correct K+ and Mg2+, overdrive pacing or isoproterenol
- Identify and treat reversible cause: ischemia (revascularize), electrolytes, drugs
Second-line / adjunct
- ICD — secondary prevention for survivors of cardiac arrest, sustained VT with structural disease, or unexplained syncope with inducible VT
- Primary prevention ICD: LVEF ≤35% on optimal GDMT (≥3 months) with NYHA II-III; LVEF ≤30% post-MI (after 40 days); selected channelopathies and high-risk HCM
- Catheter ablation — recurrent VT despite ICD, frequent appropriate shocks, idiopathic monomorphic VT (RVOT, fascicular)
- Chronic antiarrhythmic therapy: amiodarone, sotalol, mexiletine
- Beta-blocker baseline for nearly all patients with structural heart disease and VT
- Wearable cardioverter-defibrillator (LifeVest) as bridge to recovery or ICD
Complications
- Sudden cardiac death
- Anoxic brain injury after prolonged arrest
- Recurrent appropriate ICD shocks (electrical storm)
- Cardiomyopathy from incessant VT (tachycardia-mediated)
- ICD complications: lead displacement, infection, inappropriate shocks
PANCE pearls
- When in doubt about a wide-complex tachycardia, treat as VT until proven otherwise.
- AV dissociation, capture beats, and fusion beats are highly specific for VT.
- Torsades de pointes = polymorphic VT with twisting QRS axis in setting of long QT — give magnesium first.
- Brugada syndrome: pseudo-RBBB with coved ST elevation in V1-V2, autosomal dominant, risk of SCD especially at night; ICD if symptomatic.
- WPW with atrial fibrillation: AVOID AV nodal blockers (adenosine, beta-blocker, CCB, digoxin) — they accelerate the accessory pathway and can precipitate VF.
Images
References
- AHA 2020 ACLS — 2020 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Panchal et al., Circulation 2020)
- AHA/ACC/HRS 2017 VA/SCD — 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death (Al-Khatib et al., Circulation 2018)
- MADIT-II — Prophylactic Implantation of a Defibrillator in Patients with MI and Reduced EF (Moss et al., NEJM 2002)
- SCD-HeFT — Amiodarone or an ICD for Congestive Heart Failure (Bardy et al., NEJM 2005)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.