Hyperkalemia
Serum K >5.0 mEq/L; cardiac arrhythmia risk drives urgent intervention.
Also known as: hyperkalemia, high potassium
Overview
Serum potassium concentration >5.0-5.5 mEq/L (varies by lab). Severity: mild 5.5-6.0, moderate 6.1-6.9, severe ≥7.0 or any level with ECG changes. Acuity, EKG changes, and underlying cause determine urgency of intervention.
Epidemiology
Affects ~1-10% of hospitalized patients. Most common in patients with CKD, heart failure, diabetes, and those on RAAS inhibitors, MRAs, or potassium-sparing diuretics.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Hyperkalemia outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- CKD (decreased excretion)
- Medications: ACEi (lisinopril, ramipril), ARB (losartan, valsartan), MRA (spironolactone, eplerenone, finerenone), potassium-sparing diuretic (amiloride, triamterene), trimethoprim, heparin, NSAIDs, beta-blockers, digoxin (overdose)
- Type 4 RTA (hypoaldosteronism — diabetic nephropathy)
- Adrenal insufficiency (Addison disease)
- Massive cell breakdown: rhabdomyolysis, tumor lysis syndrome, hemolysis, severe burns
- Acidosis (intracellular-extracellular shift)
- Insulin deficiency / DKA
- Excessive intake (salt substitutes, supplements, transfusion of old blood)
Pathophysiology
Potassium is the major intracellular cation; only 2% extracellular. Hyperkalemia results from impaired renal excretion (CKD, hypoaldosteronism), cellular shifts (acidosis, insulin deficiency, hyperosmolality, beta-blockade, succinylcholine, digoxin toxicity), increased intake/release (rhabdomyolysis, tumor lysis), or pseudohyperkalemia (hemolyzed sample, thrombocytosis, leukocytosis). Elevated extracellular K reduces the resting membrane potential, increasing excitability initially, then impairing repolarization and conduction, ultimately causing cardiac arrest.
Clinical presentation
Symptoms
- Often asymptomatic until severe or rapidly developing
- Muscle weakness, paralysis (severe; ascending similar to Guillain-Barré)
- Paresthesias
- Palpitations, lightheadedness
- Cardiac arrest (life-threatening)
Signs / physical exam
- Often unremarkable physical exam
- Bradycardia, irregular rhythm
- Hyporeflexia, flaccid paralysis in severe cases
- Findings of underlying cause (volume status, signs of CKD, diabetic features)
Classic findings
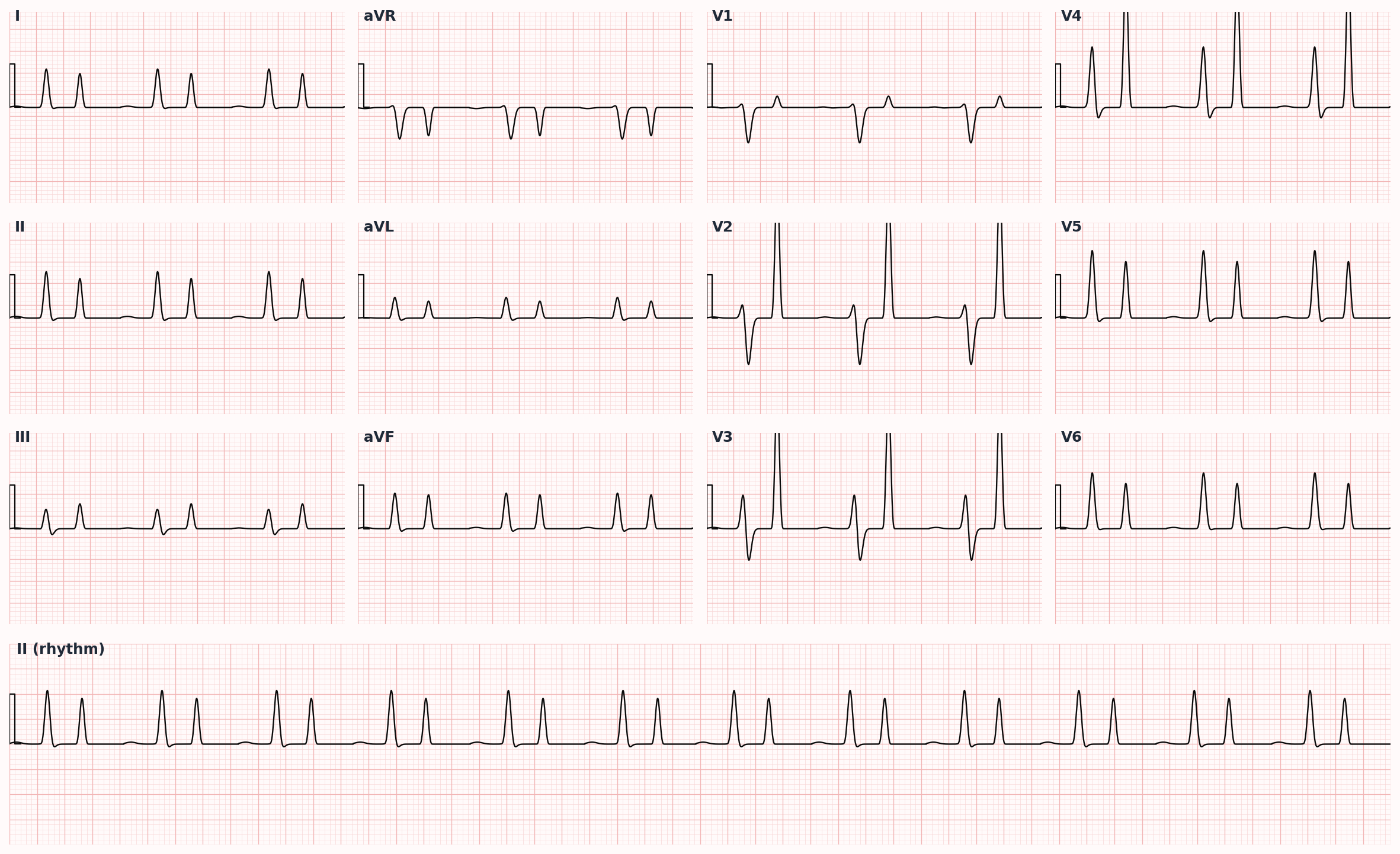
ECG progression: peaked T waves → PR prolongation → loss of P waves → wide QRS → sine wave pattern → ventricular fibrillation/asystole.
Differential diagnosis
- Pseudohyperkalemia — Hemolyzed sample, fist clenching with tourniquet, thrombocytosis, leukocytosis; repeat with non-hemolyzed sample or whole blood K
- True hyperkalemia from CKD — Elevated creatinine, known CKD; cumulative effect with ACEi/ARB/MRA
- Drug-induced — Recent ACEi/ARB/MRA/TMP-SMX initiation; review medication list
- Rhabdomyolysis / tumor lysis — Elevated CK + hyperkalemia + hyperphosphatemia + hypocalcemia + AKI
- Adrenal insufficiency — Hyperkalemia + hyponatremia + hypotension; ACTH stimulation test
- Type 4 RTA — Hyperkalemia + non-gap metabolic acidosis in diabetic; mild hyperkalemia
- DKA — Insulin deficiency shifts K out of cells; total body K is depleted despite hyperkalemia at presentation
Diagnostic workup
Diagnostic criteria
Confirmed serum K >5.0 mEq/L. ECG should be obtained urgently in any K >6.0 or any patient with cardiovascular symptoms or comorbidities.
Labs
- BMP — confirm K elevation, assess creatinine and bicarbonate
- Repeat sample if hemolysis suspected; whole blood K if pseudohyperkalemia suspected
- CBC (high WBC or platelet count may cause pseudohyperkalemia)
- ABG — assess for acidosis
- CK if rhabdomyolysis suspected
- Magnesium — concurrent low Mg makes K refractory to replacement; correct hypomagnesemia
- Urine K and urine creatinine (TTKG historical, less used) to assess renal handling
- Cortisol, aldosterone, renin if adrenal insufficiency or hypoaldosteronism suspected
- Digoxin level if applicable
Imaging
- Generally not indicated for hyperkalemia evaluation itself
Diagnostic algorithm
| Treatment | Mechanism | Onset | Duration |
|---|---|---|---|
| Calcium gluconate 1-2 g IV | Stabilizes cardiac membrane (NOT lower K) | 1-3 min | 30-60 min |
| Insulin 10 U + D50 25 g IV | Shifts K intracellularly | 15-30 min | 2-6 h |
| Albuterol 10-20 mg neb | Beta-2 driven K shift | 30 min | 2-4 h |
| Sodium bicarbonate | Shifts K (less effective in CKD) | 30-60 min | Hours |
| Furosemide IV | Renal K excretion | 30 min-2 h | Hours |
| Patiromer / Na zirconium cyclosilicate | Binds K in GI tract | 1-7 h | Sustained with daily dosing |
| Hemodialysis | Definitive K removal | Within minutes of initiation | Until next session |
Treatment
First-line
- ECG immediately — guides urgency. ECG changes or K >6.5 → emergency treatment.
- STABILIZE MEMBRANE (if ECG changes): IV calcium gluconate 1-2 g over 5-10 min (or calcium chloride 1 g via central line). Onset 1-3 min, duration 30-60 min. Repeat if no ECG improvement. CAUTION in digoxin toxicity — give slowly.
- SHIFT K INTO CELLS:
- Insulin 10 units IV + dextrose (D50 25 g) — onset 15-30 min, duration 2-6 h
- Beta-2 agonist nebulized (albuterol 10-20 mg) — onset 30 min, additive with insulin
- Sodium bicarbonate (if acidotic; less effective in CKD) — 50-100 mEq IV
- REMOVE K FROM BODY:
- Loop diuretic — furosemide, bumetanide — if kidney function and volume permit
- Potassium binder — patiromer (oral, slower onset hours), sodium zirconium cyclosilicate (oral, onset 1 h)
- Sodium polystyrene sulfonate (Kayexalate) — older agent; bowel necrosis risk especially with sorbitol; avoid in postoperative or ileus patients
- Hemodialysis — definitive treatment for ESRD or severe refractory hyperkalemia
- Stop contributing medications: ACEi/ARB/MRA, K-sparing diuretic, NSAID, TMP-SMX, supplements
Second-line / adjunct
- Treat underlying cause (DKA — insulin; rhabdomyolysis — fluids; adrenal insufficiency — steroids)
- Long-term prevention in CKD/HF: dietary K restriction, optimize diuretic, chronic potassium binder (patiromer, sodium zirconium cyclosilicate) to enable continued RAAS therapy
- Repeat K every 2-4 h until stable
- Cardiology consultation if persistent ECG changes or arrhythmia
- Recheck K and ECG after each intervention
Complications
- Cardiac arrhythmia: bradyarrhythmias, AV block, ventricular fibrillation, asystole
- Sudden cardiac death
- Muscle weakness/paralysis
- Bowel necrosis from Kayexalate (especially with sorbitol)
- Hypoglycemia from insulin treatment (monitor glucose hourly)
- Discontinuation of beneficial RAAS therapy in heart failure / CKD without binders
PANCE pearls
- Order of treatment in severe hyperkalemia: STABILIZE (calcium) → SHIFT (insulin/dextrose, beta-agonist, bicarbonate) → REMOVE (diuretic, binder, dialysis). 'C-BIG-K-Drop' mnemonic.
- Calcium gluconate STABILIZES the cardiac membrane but does NOT lower potassium. Calcium chloride has 3× the elemental calcium of gluconate but causes tissue necrosis if extravasated.
- Insulin + dextrose temporarily shifts K into cells but does not eliminate it; total body K unchanged.
- Kayexalate (SPS) has limited efficacy and notable risk of intestinal necrosis. Patiromer and sodium zirconium cyclosilicate are preferred modern alternatives.
- Pseudohyperkalemia clues: hemolyzed sample (mention by lab), discrepancy between serum and plasma K, severe thrombocytosis or leukocytosis. Always confirm before invasive treatment.
- Patients with CKD or HF on ACEi/ARB benefit from chronic K binder therapy to maintain RAAS blockade — KDIGO 2024 endorsement.
Images
References
- KDIGO 2020 — KDIGO Controversies Conference on Potassium Management in Kidney Disease
- AHA 2020 — AHA Adult Advanced Cardiac Life Support Guidelines (hyperkalemia in cardiac arrest)
- Lindner et al. 2020 — Acute Hyperkalemia in the Emergency Department (J Emerg Med 2020)
Practice Renal/Urology questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.