Atrial Flutter
Macro-reentrant atrial tachycardia with sawtooth flutter waves; treated like AFib for stroke risk.
Also known as: AFlutter, flutter, atrial flutter, sawtooth, cavotricuspid isthmus
Overview
Organized macro-reentrant atrial tachycardia, typically with atrial rates 250-350 bpm (usually ~300), producing characteristic sawtooth flutter waves on ECG. Ventricular response depends on AV node conduction ratio (2:1, 3:1, 4:1).
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Atrial Flutter outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Pathophysiology
Typical (counterclockwise) flutter: re-entrant circuit travels counterclockwise around the tricuspid annulus, with critical conduction through the cavotricuspid isthmus (CTI) at the floor of the right atrium. This anatomic substrate makes CTI ablation curative. Atypical flutter has variable circuits, often in the left atrium post-ablation or post-cardiac surgery.
Clinical presentation
Symptoms
- Often more symptomatic than AFib due to faster, regular ventricular rates
- Palpitations, dyspnea, exercise intolerance
- Lightheadedness, chest discomfort
- May present as new HF or with embolic stroke
Signs / physical exam
- Regular tachycardia (in contrast to AFib's irregularly irregular)
- Ventricular rate often a fixed multiple — 150 bpm (2:1), 100 (3:1), 75 (4:1)
- Cannon a waves may be seen in JVP
- Carotid massage or adenosine transiently blocks AV node — unmasks flutter waves diagnostically
Classic findings
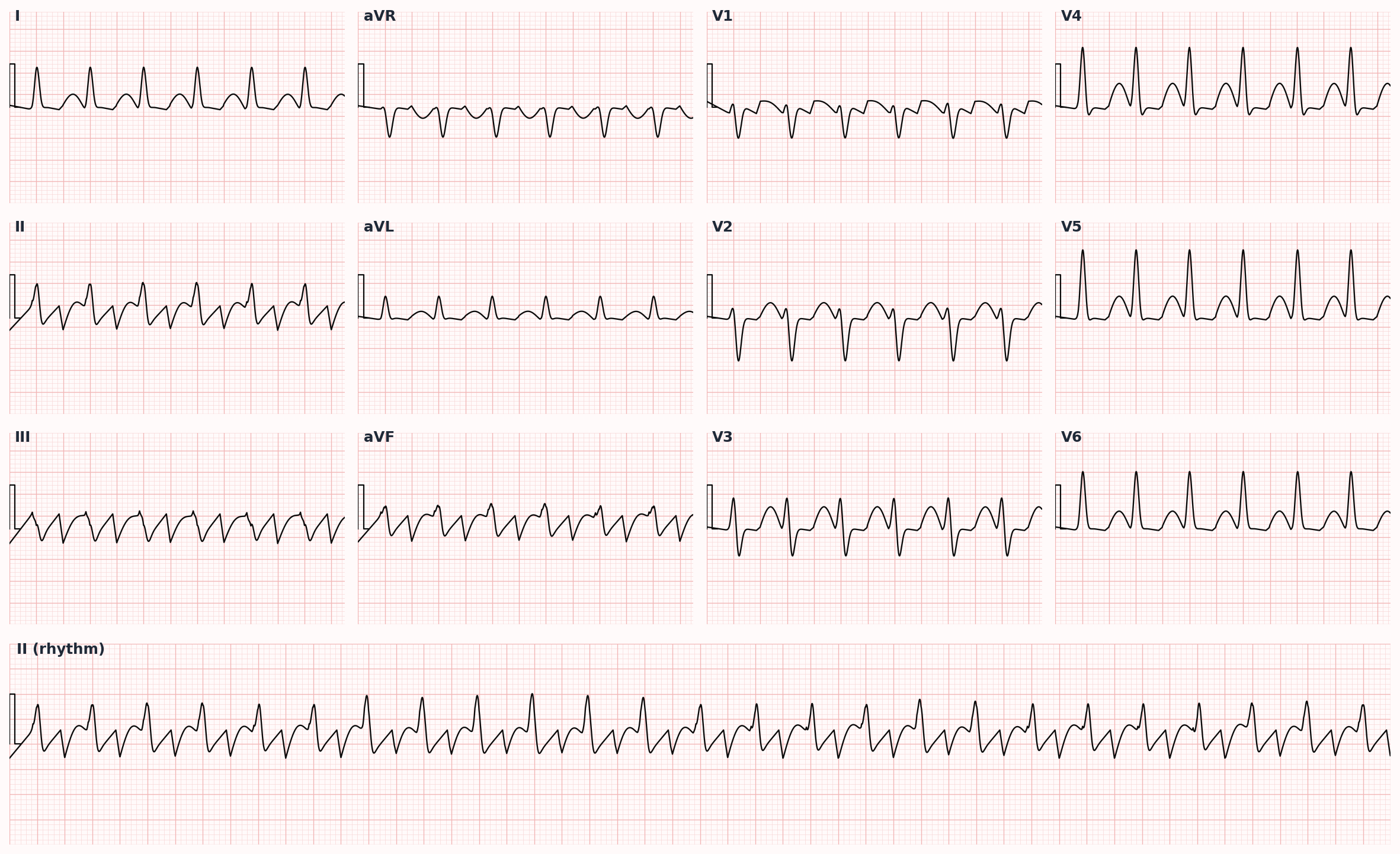
ECG: 'sawtooth' flutter waves (negative deflections in II, III, aVF and positive in V1) in typical counterclockwise flutter.
Differential diagnosis
- Atrial fibrillation (rate-controlled) — AFib at controlled rates can appear regular; absent P waves and fibrillatory baseline distinguish from flutter waves
- AV nodal reentrant tachycardia (AVNRT) — Narrow-complex regular tachycardia, abrupt onset/offset, often 150-220 bpm; vagal maneuvers or adenosine terminate; pseudo-R' in V1 from retrograde P
- AV reentrant tachycardia (AVRT, e.g., WPW) — Narrow-complex (orthodromic) or wide-complex (antidromic); delta wave visible in baseline sinus rhythm; AVOID AV-nodal blockers if pre-excited AFib
- Sinus tachycardia at high rate — Gradual onset, identifiable trigger (fever, hypovolemia, anxiety, anemia), visible P waves with normal morphology
- Focal atrial tachycardia — Single ectopic P-wave morphology different from sinus; rate 130-180 typically; less rapid than flutter
- Ventricular tachycardia — Wide-complex; AV dissociation, capture/fusion beats, RBBB-like morphology >140 ms; assume VT until proven otherwise in patient with structural heart disease
Diagnostic workup
Labs
- TSH, CBC, BMP, magnesium
- Coagulation studies
- Troponin if ischemia in differential
Imaging
- 12-lead ECG — diagnostic when flutter waves visible; 2:1 conduction can hide them (rate 150 should prompt vagal maneuvers or adenosine to unmask)
- TTE for LA size, LV function, valve disease
- TEE prior to cardioversion if duration unknown/>48 h and not adequately anticoagulated
Diagnostic algorithm
| Feature | Atrial Fibrillation | Atrial Flutter |
|---|---|---|
| Atrial rate | 350-600 bpm (chaotic) | 250-350 bpm (~300 typical) |
| Ventricular rhythm | Irregularly irregular | Regular (or regularly irregular with variable block) |
| P waves | Absent — fibrillatory baseline | Sawtooth flutter waves (II, III, aVF negative in typical) |
| Typical ventricular rate | 100-160 (variable) | 150 (2:1), 100 (3:1), 75 (4:1) |
| Anticoagulation | CHA2DS2-VASc-driven | Same — equivalent stroke risk |
| Cardioversion energy | 120-200 J biphasic | 50-100 J biphasic |
| Curative ablation | PVI — ~70-80% success | CTI ablation — >90% success |
| AFib often follows ablation? | — | Yes (~30% over years) |
Treatment
First-line
- Acute rate control: same as AFib — IV beta-blocker or non-DHP CCB
- Anticoagulation: same CHA2DS2-VASc-based decision as AFib (flutter carries equivalent stroke risk)
- Cardioversion (synchronized DCCV) — flutter typically cardioverts at lower energy (50-100 J biphasic) than AFib (120-200 J)
- Definitive: catheter ablation of cavotricuspid isthmus is curative for typical flutter with >90% success and low recurrence — preferred first-line in many patients
Second-line / adjunct
- Antiarrhythmics (less effective than for AFib): ibutilide acutely; dofetilide, sotalol, amiodarone for maintenance
- If cardioversion repeatedly fails or recurs despite AAD, refer for ablation
- AFib commonly emerges after flutter ablation (~30% over years) — counsel patients and continue anticoagulation per CHA2DS2-VASc regardless of rhythm status
Complications
- Embolic stroke (equivalent risk to AFib)
- Tachycardia-induced cardiomyopathy (rapid 1:1 or 2:1 conduction sustained)
- Heart failure
- 1:1 conduction with class IC antiarrhythmic (flecainide) — paradoxical rate acceleration; always pair flecainide with an AV nodal blocker
PANCE pearls
- Regular narrow-complex tachycardia at exactly 150 bpm is atrial flutter with 2:1 conduction until proven otherwise. Use vagal maneuvers or adenosine to unmask the flutter waves diagnostically (not therapeutically).
- CTI ablation has the highest success rate of any cardiac ablation procedure — counsel as first-line for most patients with typical flutter.
- Apply the same stroke-prevention rules as AFib — flutter is NOT lower-risk for embolism despite being a more organized rhythm.
- Atypical flutter often arises from prior left atrial ablation scars (post-PVI for AFib) — these require complex 3D mapping for ablation.
Images
References
- ACC/AHA/HRS 2015 SVT — 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia (Page et al., Circulation 2016)
- ACC/AHA/ACCP/HRS 2023 — 2023 AFib Guideline applies same anticoagulation principles to flutter (Joglar et al., Circulation 2024)
- Cosío 2017 — Atrial Flutter, Typical and Atypical: A Review (Cosío, Arrhythm Electrophysiol Rev 2017)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.