Hypertension
Persistently elevated BP ≥130/80 (ACC/AHA 2017); cornerstone modifiable cardiovascular risk factor.
Also known as: HTN, high blood pressure, essential hypertension, primary hypertension
Overview
Sustained elevation of arterial blood pressure ≥130/80 mmHg (ACC/AHA 2017 thresholds) based on average of ≥2 properly measured readings on ≥2 occasions. Stage 1: 130-139/80-89. Stage 2: ≥140/90. Hypertensive crisis: ≥180/120 (urgency if no end-organ damage; emergency if present).
Epidemiology
Affects nearly half of US adults under current guidelines. Leading modifiable risk factor for cardiovascular disease, stroke, CKD, and dementia worldwide.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Hypertension outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Non-modifiable: age, family history, Black race (earlier onset, more severe)
- Modifiable: high sodium diet, low potassium intake, obesity, sedentary lifestyle, alcohol use, smoking, chronic stress, poor sleep / OSA
- Secondary causes (~5-10% of cases) to consider especially in young, resistant, or rapidly accelerating HTN:
- • Renal: renal artery stenosis (FMD in young women; atherosclerotic in older), CKD, glomerular disease
- • Endocrine: primary hyperaldosteronism (Conn's — low K, metabolic alkalosis), pheochromocytoma (paroxysmal HTN, headache, sweating, palpitations), Cushing syndrome, hyperthyroidism
- • Coarctation of aorta — upper-extremity HTN, lower-extremity hypotension, radio-femoral delay
- • Obstructive sleep apnea (very common, under-recognized)
- • Medications: NSAIDs, OCPs, decongestants, stimulants, SNRIs
Pathophysiology
Multifactorial: increased peripheral vascular resistance from inappropriate RAAS activation, sympathetic overactivity, endothelial dysfunction, vascular remodeling, and renal sodium handling abnormalities. Genetic predisposition interacts with dietary and lifestyle exposures.
Clinical presentation
Symptoms
- Almost always asymptomatic — 'silent killer'
- Severe HTN may produce: occipital headache, blurred vision, epistaxis, chest discomfort
- Hypertensive emergency: neurologic deficits, chest pain (dissection, MI), dyspnea (flash pulmonary edema), oliguria
Signs / physical exam
- Elevated office BP — confirm with ambulatory or home BP monitoring (rule out white-coat HTN)
- Funduscopy: AV nicking, copper/silver wiring, hemorrhages, exudates, papilledema (hypertensive retinopathy stages I-IV)
- Cardiac: S4 gallop from LVH; lateral PMI
- Abdominal bruit (renovascular disease)
- Asymmetric pulses or BP arm-to-arm differences (suggest dissection or coarctation)
Differential diagnosis
- White-coat hypertension — Office BP elevated, ambulatory or home BP normal; ~20% of office HTN patients; no end-organ damage on workup
- Masked hypertension — Office BP normal, out-of-office BP elevated; carries worse cardiovascular prognosis than white-coat; suspect with end-organ damage despite 'normal' office readings
- Pseudohypertension (elderly) — Calcified non-compressible arteries cause falsely elevated cuff readings; persistent palpable radial pulse with cuff inflated above SBP (Osler maneuver)
- Renal artery stenosis — Abdominal bruit, refractory HTN, ↑ creatinine after ACEi/ARB; FMD in young women, atherosclerotic in older men; renal artery Doppler or MRA
- Primary hyperaldosteronism (Conn syndrome) — Hypokalemia, metabolic alkalosis, suppressed renin, elevated aldosterone-to-renin ratio; adrenal CT
- Pheochromocytoma — Paroxysmal HTN with the '5 H's' — headache, hypertension, hyperhidrosis, heart palpitations, hyperglycemia; plasma or 24-h urine metanephrines
- Cushing syndrome — Central obesity, moon facies, abdominal striae, easy bruising, proximal muscle weakness; 24-h urine free cortisol or dexamethasone suppression
- Coarctation of the aorta — Upper-extremity HTN with weak/delayed femoral pulses; radio-femoral delay; rib notching on CXR (children/young adults)
- Obstructive sleep apnea — Snoring, witnessed apneas, daytime somnolence, obesity; polysomnography; CPAP can lower BP
- Drug or substance-induced — NSAIDs, OCPs, decongestants (pseudoephedrine), stimulants (cocaine, amphetamines), SNRIs, corticosteroids, licorice (mineralocorticoid effect)
Diagnostic workup
Labs
- BMP (Cr, K, glucose), UA with albumin-to-creatinine ratio
- Lipid panel, A1c, TSH
- CBC
- If secondary HTN suspected: aldosterone-to-renin ratio, 24-h urine metanephrines, renal artery Doppler/MRA, polysomnography
Imaging
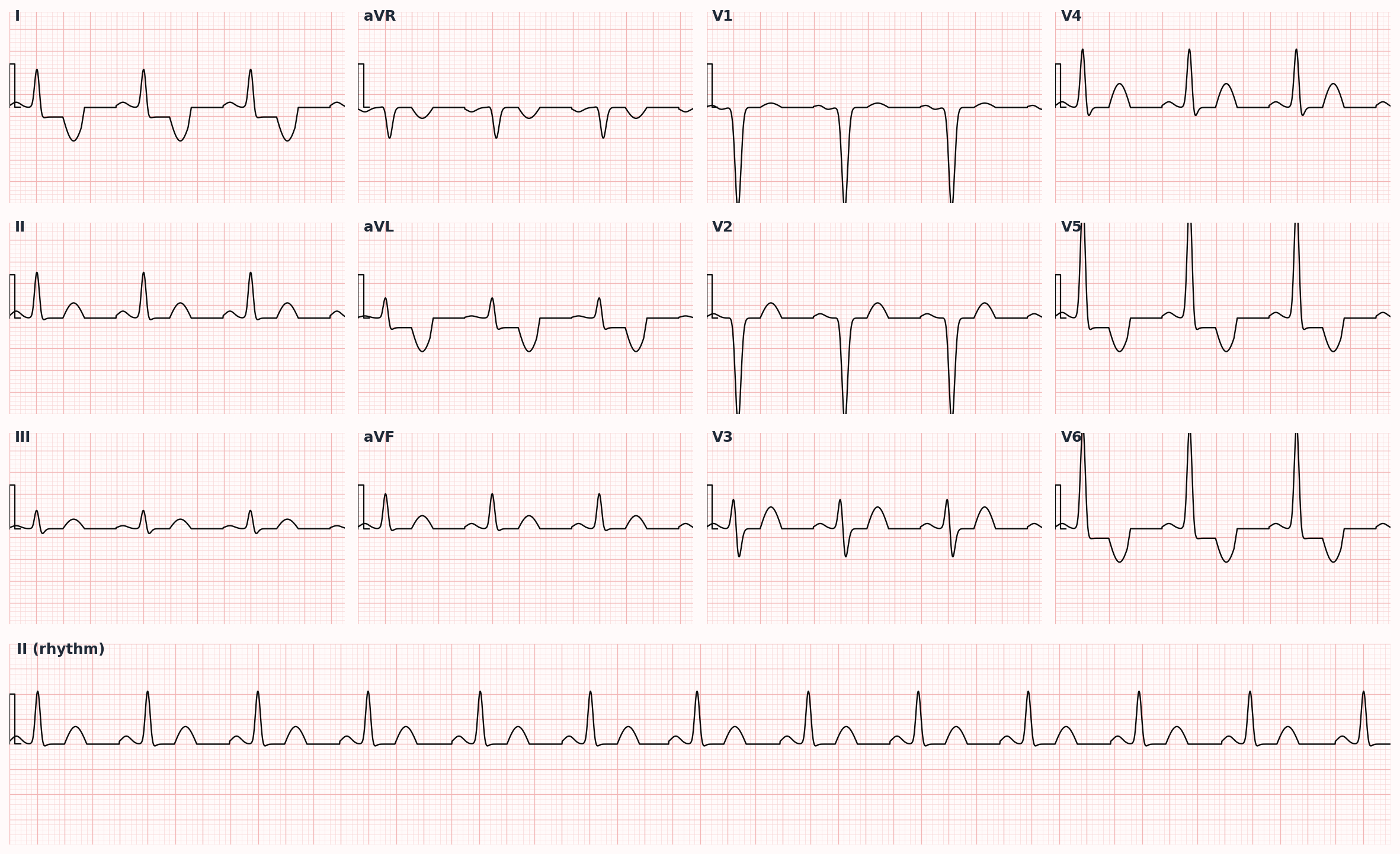
- 12-lead ECG — LVH (Cornell or Sokolow-Lyon criteria), prior MI
- Echocardiogram if LVH on ECG, HF symptoms, or diagnostic uncertainty
Diagnostic algorithm
| Compelling Indication | Preferred First-Line Class |
|---|---|
| Heart failure (HFrEF) | ACEi/ARB + beta-blocker (evidence-based) + MRA + diuretic |
| Post-MI / CAD | Beta-blocker + ACEi/ARB |
| Diabetes mellitus | ACEi or ARB (renal protection) |
| CKD with proteinuria | ACEi or ARB |
| Recurrent stroke prevention | Thiazide diuretic + ACEi |
| Black race (no compelling indication) | Thiazide diuretic or CCB |
| Pregnancy | Labetalol, nifedipine, methyldopa (AVOID ACEi/ARB — teratogenic) |
| Resistant HTN (>3 drugs incl. diuretic) | Add spironolactone; investigate secondary causes |
Treatment
First-line
- Lifestyle modifications (always foundational):
- • DASH diet — fruits, vegetables, whole grains, low-fat dairy
- • Sodium <1500-2000 mg/day
- • Weight loss (each 1 kg ≈ 1 mmHg drop)
- • Aerobic exercise 150 min/week moderate intensity
- • Alcohol limit (≤2 drinks/day men, ≤1 women)
- • Smoking cessation
- Pharmacologic — initiate if stage 1 + ASCVD risk ≥10%, established CVD, DM, or CKD; or stage 2 regardless:
- • First-line classes (any of, by representative agent):
- • Thiazide diuretic — chlorthalidone (preferred over HCTZ for stronger CV outcome data), HCTZ, indapamide
- • ACE inhibitor — lisinopril, enalapril, ramipril, benazepril
- • ARB — losartan, valsartan, candesartan, telmisartan, irbesartan
- • Dihydropyridine CCB — amlodipine, nifedipine ER, felodipine
- • Black patients without HF/CKD: CCB or thiazide preferred first-line over ACEi/ARB monotherapy
Second-line / adjunct
- Combination therapy if BP >20/10 mmHg above goal at diagnosis (start 2 drugs)
- Add second drug from different class if monotherapy insufficient
- Compelling indications (drug choice driven by comorbidity):
- • HFrEF: ACEi or ARB + BB + MRA + diuretic
- • Post-MI: BB + ACEi/ARB
- • CKD with proteinuria: ACEi or ARB
- • Diabetes: ACEi or ARB
- • Recurrent stroke prevention: thiazide + ACEi
- • BPH: alpha-blocker (doxazosin) — symptomatic relief but NOT first-line for HTN alone (ALLHAT)
- Resistant HTN (BP uncontrolled on 3 drugs including a diuretic): add spironolactone (PATHWAY-2 trial); investigate secondary causes
Complications
- Atherosclerotic cardiovascular disease: MI, stroke, peripheral arterial disease
- Hypertensive heart disease: LVH → HFpEF → HFrEF, AFib
- Chronic kidney disease — second leading cause of ESRD after diabetes
- Hypertensive retinopathy
- Aortic dissection
- Hypertensive emergency with end-organ damage (encephalopathy, pulmonary edema, AKI)
PANCE pearls
- Proper BP measurement: seated, back supported, feet flat, arm at heart level, no caffeine/exercise/smoking 30 min prior, appropriate cuff size. Average of ≥2 readings on ≥2 occasions.
- ACEi cough (10-20% of patients, bradykinin-mediated) → switch to ARB. Angioedema → avoid both ACEi AND ARB (cross-reactivity ~10%).
- Hypertensive urgency (≥180/120 no end-organ damage): oral therapy, gradual reduction over 24-48 h. Hypertensive emergency: IV therapy, reduce MAP 10-20% in first hour, then more gradually. Acute dissection: aggressive — SBP <120 in minutes.
- Avoid sublingual nifedipine — unpredictable, can cause stroke or MI from rapid hypotension. Pulled from US market for this use decades ago.
- Lower 'goal' to <130/80 in most patients per SPRINT (intensive control reduces CV events but increases AKI, syncope, electrolyte abnormalities).
Images
References
- ACC/AHA 2017 — 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults (Whelton et al., Hypertension 2018)
- SPRINT — A Randomized Trial of Intensive versus Standard Blood-Pressure Control (SPRINT Research Group, NEJM 2015)
- ALLHAT — Major Outcomes in High-Risk Hypertensive Patients Randomized to ACEi, CCB, or Thiazide (ALLHAT Officers, JAMA 2002)
- PATHWAY-2 — Spironolactone vs Placebo, Bisoprolol, Doxazosin for Resistant HTN (Williams et al., Lancet 2015)
- JNC 8 — 2014 Evidence-Based Guideline for the Management of High Blood Pressure (James et al., JAMA 2014)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.