Acute Coronary Syndrome (ACS)
Spectrum of acute myocardial ischemia: unstable angina → NSTEMI → STEMI.
Also known as: ACS, MI, myocardial infarction, STEMI, NSTEMI, unstable angina, heart attack
Overview
Spectrum of clinical syndromes resulting from acute myocardial ischemia, classified by ECG and biomarker findings: ST-elevation MI (STEMI), non-ST-elevation MI (NSTEMI), and unstable angina (UA).
Epidemiology
Leading cause of death in the US. Incidence rises sharply with age; male predominance until ~70 when rates equalize.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Acute Coronary Syndrome (ACS) outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Non-modifiable: age, male sex, family history of premature CAD (<55 men / <65 women)
- Modifiable: smoking, diabetes, hypertension, dyslipidemia, obesity, sedentary lifestyle
- Other: chronic kidney disease, autoimmune disease, cocaine/methamphetamine use
Pathophysiology
Atherosclerotic plaque rupture or erosion exposes thrombogenic material to circulating blood, triggering platelet aggregation and thrombus formation. Partial occlusion → UA/NSTEMI. Complete occlusion → STEMI. Resulting downstream ischemia → myocyte necrosis if not reperfused.
Clinical presentation
Symptoms
- Substernal chest pressure, tightness, or 'heaviness' (classic), often radiating to left arm, jaw, or back
- Dyspnea, diaphoresis, nausea/vomiting
- Atypical in women, elderly, diabetics: fatigue, epigastric pain, syncope, dyspnea without pain
- Symptoms ≥20 min and not relieved by rest/nitrates suggest infarction
Signs / physical exam
- Diaphoresis, anxiety, hypotension or hypertension
- S4 gallop (LV stiffness from ischemia)
- New MR murmur → papillary muscle dysfunction
- Crackles → LV failure
Classic findings
Levine's sign (clenched fist over sternum); cool/clammy skin; bradycardia in inferior MI.
Differential diagnosis
- Aortic dissection — Sudden tearing or ripping chest pain radiating to the back, BP or pulse differential between arms, widened mediastinum on CXR — DO NOT anticoagulate before excluding
- Pulmonary embolism — Sudden pleuritic chest pain, dyspnea, hypoxia, risk factors (immobility, malignancy, OCPs); RV strain on ECG/echo; D-dimer / CTPA
- Pericarditis / myopericarditis — Sharp pleuritic pain improved leaning forward, diffuse concave ST elevation with PR depression, friction rub, recent viral illness
- Takotsubo (stress) cardiomyopathy — Postmenopausal women after major emotional/physical stressor; ECG and troponin mimic STEMI; apical ballooning on ventriculogram or echo
- Tension pneumothorax — Acute dyspnea, unilateral absent breath sounds, tracheal deviation, hypotension — clinical diagnosis; do not delay decompression for CXR
- Esophageal rupture (Boerhaave) — Severe chest/upper abdominal pain after forceful emesis, subcutaneous emphysema, pneumomediastinum on imaging
- GERD / esophageal spasm — Burning, postprandial, worse supine; may respond to nitrates and confuse the picture; PPI trial
- Costochondritis / musculoskeletal — Reproducible with chest wall palpation, no exertional pattern, normal ECG and troponin
Diagnostic workup
Diagnostic criteria
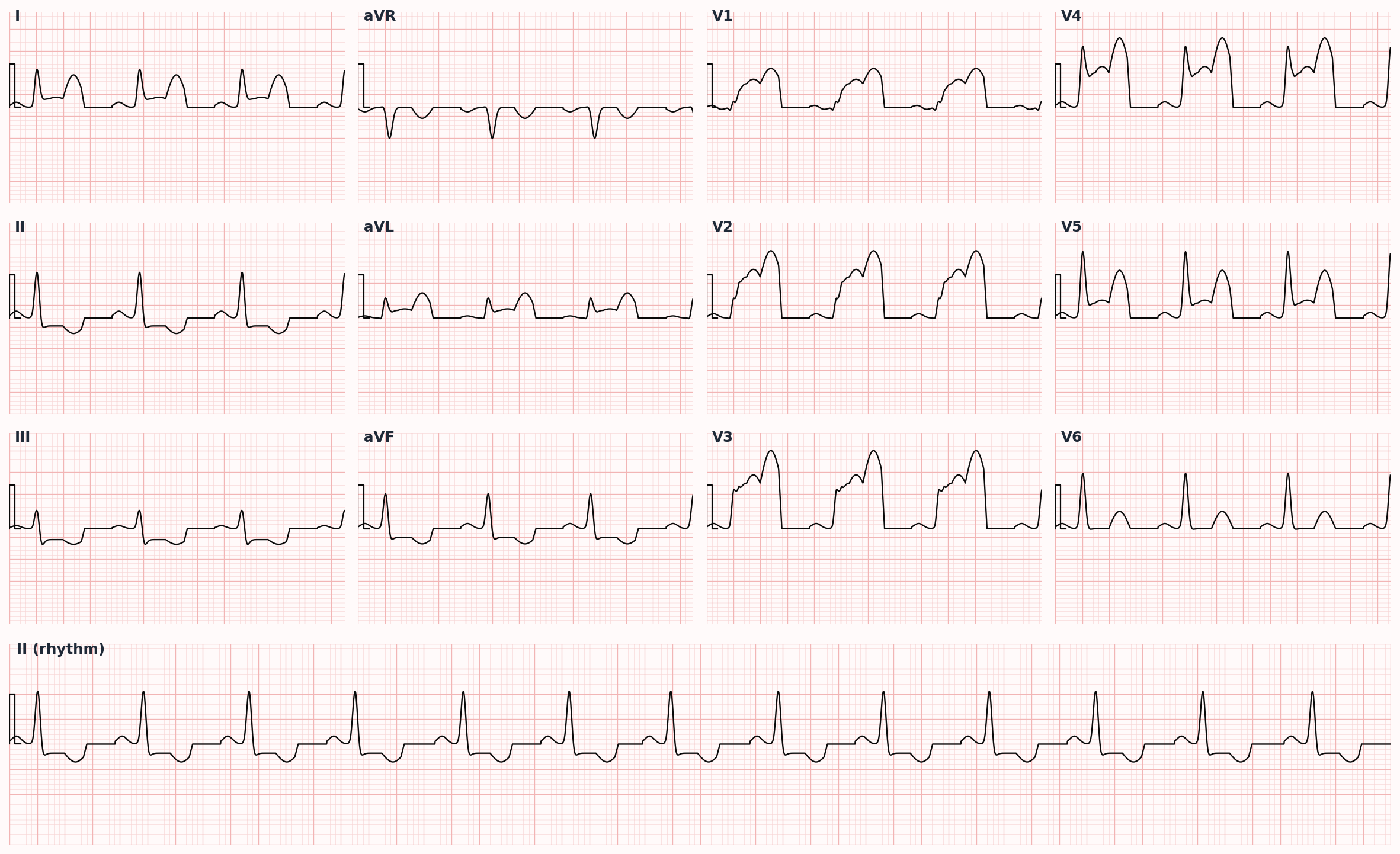
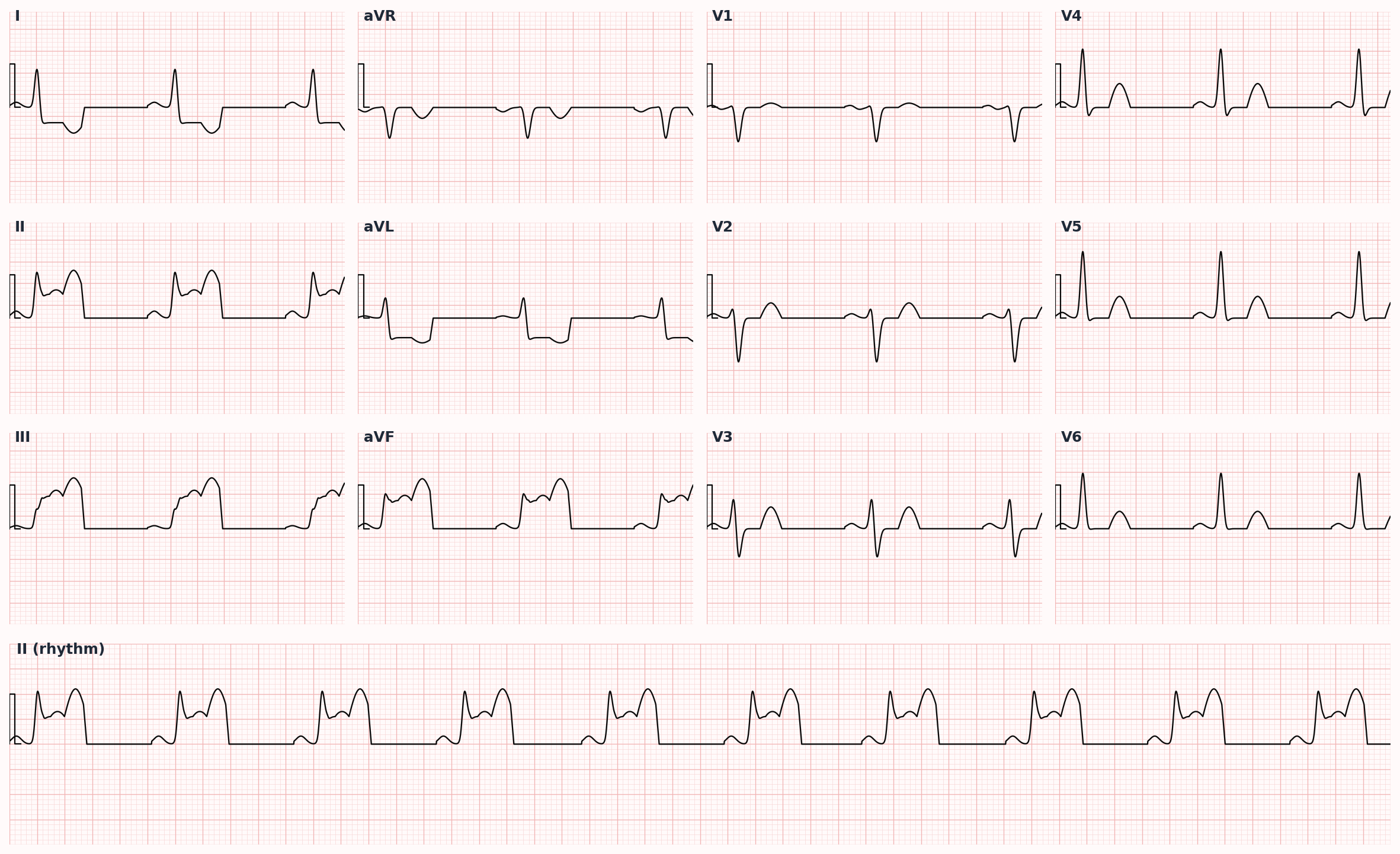
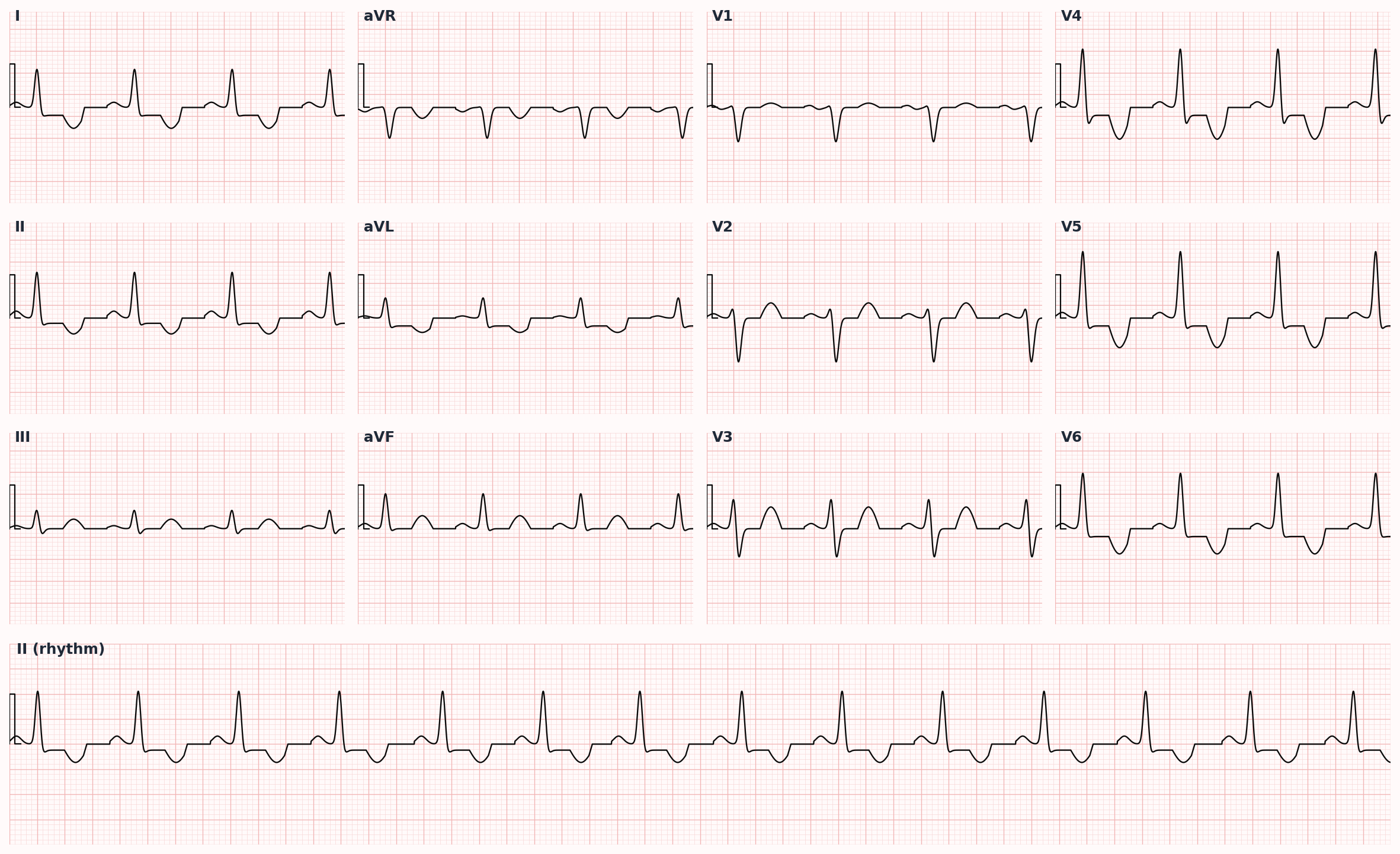
STEMI: ≥1 mm ST elevation in 2 contiguous limb leads OR ≥2 mm in 2 contiguous precordial leads (V2-V3 thresholds vary by age/sex), or new LBBB with clinical correlation. NSTEMI: positive troponin + ischemic symptoms ± ST depression / T-wave inversion. UA: ischemic symptoms with negative troponin.
Labs
- Troponin I or T (high-sensitivity) at presentation and 1-3 hours later — single most important biomarker
- CBC, BMP, Mg, lipid panel, A1c
- Coagulation studies prior to antiplatelet/anticoagulant therapy
Imaging
- 12-lead ECG within 10 minutes of arrival — repeat every 15-30 min if initial nondiagnostic
- Portable CXR (look for pulmonary edema, widened mediastinum to exclude aortic dissection)
- Bedside echo if hemodynamic instability or mechanical complication suspected
Diagnostic algorithm
flowchart TD
A[Chest pain<br/>≥10 min, suggestive] --> B[12-lead ECG<br/>within 10 min]
B --> C{ST elevation?}
C -->|Yes| D[STEMI]
D --> E[Primary PCI<br/>≤90 min]
D --> F[Fibrinolysis<br/>if PCI delay]
C -->|No| G[Troponin<br/>0 and 1-3 h]
G --> H{Troponin<br/>elevated?}
H -->|Yes| I[NSTEMI]
I --> J[Risk stratify<br/>TIMI / GRACE]
J --> K[Early invasive<br/>≤24 h if high risk]
H -->|No| L{Ongoing<br/>ischemic Sx?}
L -->|Yes| M[Unstable Angina]
M --> N[Medical optimization<br/>+ stress test]
L -->|No| O[Non-cardiac<br/>workup]Treatment
First-line
- Aspirin 325 mg chewed immediately
- P2Y12 inhibitor loading dose: ticagrelor 180 mg, clopidogrel 600 mg, or prasugrel 60 mg (prasugrel only if known anatomy proceeding to PCI; avoid if age >75, weight <60 kg, or prior stroke/TIA)
- Anticoagulation: unfractionated heparin (preferred for PCI), enoxaparin, bivalirudin, or fondaparinux (NSTEMI medical management)
- High-intensity statin on admission regardless of baseline LDL — atorvastatin 40-80 mg or rosuvastatin 20-40 mg
- Beta-blocker within 24 h (oral): metoprolol tartrate or succinate, carvedilol, or bisoprolol — avoid in acute decompensated HF, bradycardia, hypotension
- Sublingual nitroglycerin for ongoing pain (avoid in inferior/RV infarct, hypotension, recent PDE5 inhibitor use)
- Supplemental O2 only if SpO2 <90% (routine O2 worsens outcomes in normoxic patients)
STEMI
- Primary PCI within 90 min of first medical contact (preferred)
- Fibrinolysis (alteplase, tenecteplase) if PCI unavailable within 120 min and symptom onset <12 h
- Door-to-needle goal ≤30 min for fibrinolysis
NSTEMI / High-risk UA
- Risk-stratify with TIMI or GRACE score
- Early invasive (cath <24 h) for GRACE >140, refractory ischemia, hemodynamic/electrical instability, new HF
- Delayed invasive (cath 24-72 h) for intermediate risk
Low-risk UA
- Conservative strategy: medical optimization + stress testing prior to discharge
- Cath if stress test positive or symptoms recur
Second-line / adjunct
- ACEi/ARB within 24 h if LV dysfunction, anterior MI, HTN, diabetes, or CKD
- Aldosterone antagonist (spironolactone, eplerenone) if EF ≤40% + symptoms or diabetes
- Cardiac rehab referral at discharge
Complications
- Arrhythmias: ventricular fibrillation (early, most common cause of death pre-hospital), AV blocks (especially inferior MI), atrial fibrillation
- Mechanical (days 3-7): papillary muscle rupture (acute MR), ventricular septal rupture, free wall rupture (tamponade)
- Heart failure (acute or chronic), cardiogenic shock
- LV thrombus → embolic stroke (especially large anterior MI)
- Dressler syndrome (post-MI pericarditis, 2-10 weeks): pleuritic chest pain, fever, friction rub
PANCE pearls
- Posterior MI = ST depression in V1-V3 with prominent R wave (mirror image). Obtain posterior leads V7-V9.
- Inferior MI (II, III, aVF) with RV involvement (V4R) — preload-dependent. NITRATES AND DIURETICS ARE CONTRAINDICATED. Give IV fluids.
- Wellens syndrome: biphasic or deep symmetric T-wave inversions in V2-V3 = critical proximal LAD stenosis. Often pain-free at presentation. Stress testing contraindicated; cath directly.
- New LBBB with chest pain is treated as STEMI equivalent if Sgarbossa criteria positive.
- Cocaine-induced MI: avoid beta-blockers (unopposed alpha vasoconstriction). Use benzodiazepines, nitrates, CCBs.
Images
References
- ACC/AHA/SCAI 2021 — 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization (Lawton et al., Circulation 2022)
- AHA/ACC 2014 — AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes (Amsterdam et al., JACC 2014)
- ACCF/AHA 2013 — ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction (O'Gara et al., JACC 2013)
- Universal Definition — Fourth Universal Definition of Myocardial Infarction (Thygesen et al., JACC 2018)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.