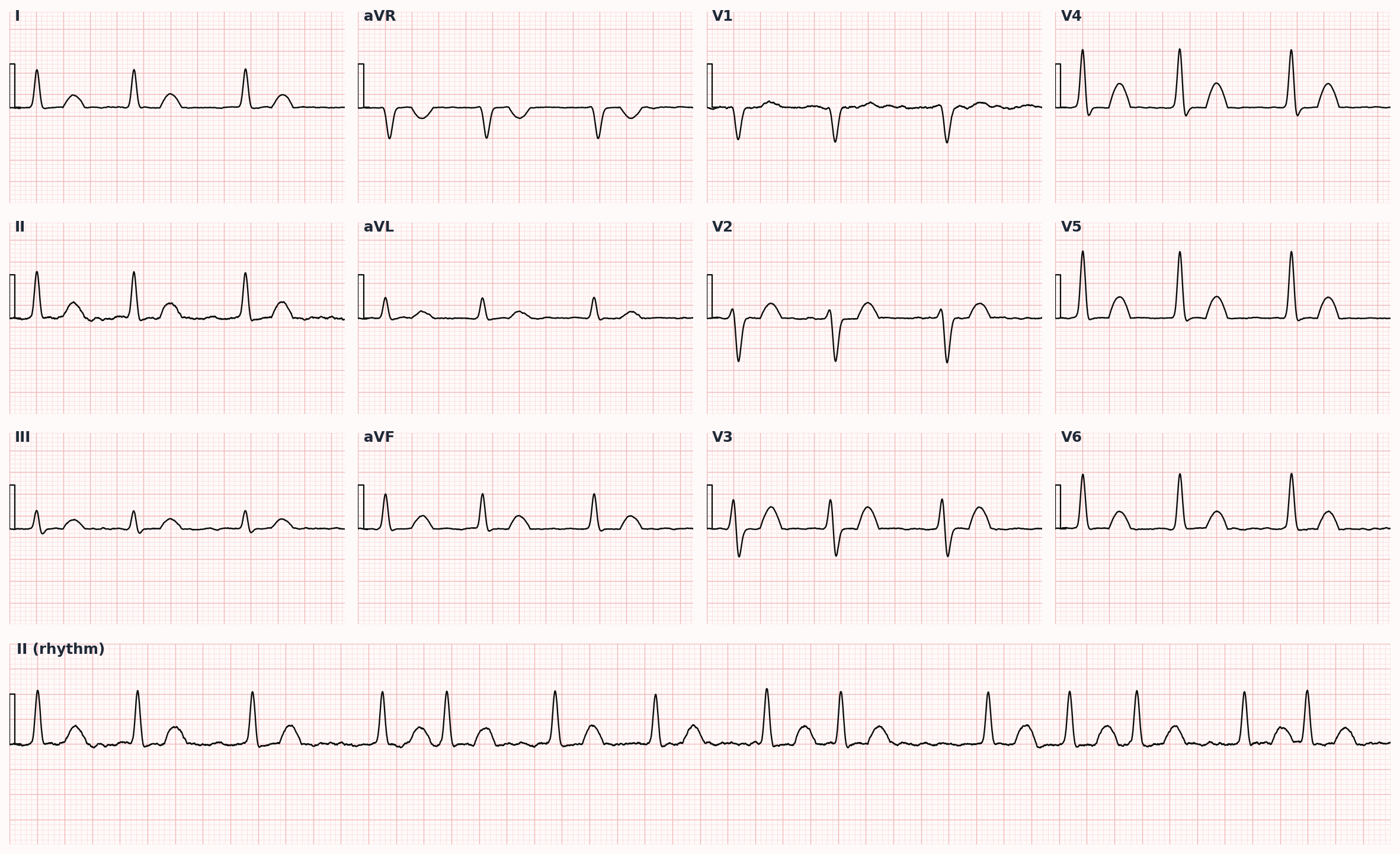
Atrial Fibrillation
Most common sustained arrhythmia: irregularly irregular rhythm with no discrete P waves.
Also known as: AFib, AF, atrial fibrillation, irregularly irregular
Overview
Supraventricular tachyarrhythmia with chaotic atrial activation, producing an irregularly irregular ventricular response and absent discrete P waves on ECG. Classified as paroxysmal (terminates <7 days), persistent (>7 days requiring intervention), long-standing persistent (>12 months), or permanent (decision made not to restore sinus rhythm).
Epidemiology
Most common sustained arrhythmia. Prevalence rises sharply with age — ~10% in adults >80. Lifetime risk ~1 in 3 after age 55.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Atrial Fibrillation outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Hypertension (most common identifiable cause)
- Coronary artery disease, valvular disease (especially mitral)
- Hyperthyroidism — always check TSH on new diagnosis
- Obesity, obstructive sleep apnea
- Alcohol use ('holiday heart'), stimulants
- Diabetes, CKD
- Pericarditis, recent cardiac surgery
Pathophysiology
Ectopic foci, typically arising from the pulmonary vein ostia, trigger multiple re-entrant wavelets in remodeled atrial tissue. Loss of organized atrial contraction reduces cardiac output by ~20% (loss of atrial kick) and promotes thrombus formation in the left atrial appendage — the substrate for embolic stroke.
Clinical presentation
Symptoms
- Palpitations (most common)
- Dyspnea, fatigue, exercise intolerance
- Lightheadedness, presyncope; rarely syncope
- Often asymptomatic — found incidentally on exam or wearable device
- Acute presentation may be embolic stroke or decompensated HF
Signs / physical exam
- Irregularly irregular pulse — pathognomonic on exam
- Pulse deficit (apical-radial mismatch)
- Variable S1 intensity beat-to-beat
- Absent a-wave in JVP
Differential diagnosis
- Atrial flutter with variable AV block — Sawtooth flutter waves (II, III, aVF) identify; can mimic AFib's irregularity when conduction ratio varies
- Multifocal atrial tachycardia (MAT) — ≥3 distinct P-wave morphologies in same lead; typically COPD or hypoxic patient; treat underlying cause + non-DHP CCB
- Atrial tachycardia with variable AV block — Single ectopic P-wave morphology (different from sinus); variable AV conduction creates irregularity
- Frequent premature atrial contractions (PACs) — Irregular rhythm but discrete P waves visible (often abnormal morphology); usually benign in structurally normal hearts
- Ventricular bigeminy or trigeminy — Wide-complex pattern with regular sequence; PVC after each (or every other) sinus beat
- Sinus arrhythmia — Phasic variation with respiration in young/healthy patients; P-wave morphology preserved
- Wandering atrial pacemaker — ≥3 P-wave morphologies but rate <100 (vs MAT >100); usually benign
Diagnostic workup
Labs
- TSH (thyrotoxicosis), CBC, BMP, magnesium
- Troponin if ischemia suspected
- Coagulation studies prior to anticoagulation
Imaging
- 12-lead ECG: irregularly irregular RR, no P waves, narrow QRS (unless aberrancy/pre-existing BBB)
- Holter or event monitor for paroxysmal AFib not captured on ECG
- TTE: LA size, LV function, valve disease, LVH
- TEE prior to cardioversion if >48 h duration or unknown onset and not therapeutically anticoagulated for ≥3 weeks
Diagnostic algorithm
flowchart TD
A[New AFib<br/>diagnosis] --> B[Calculate<br/>CHA2DS2-VASc]
B --> C{Score}
C -->|Men ≥2<br/>Women ≥3| D[Anticoagulate]
C -->|Men 0-1<br/>Women 0-2| E[Reassess<br/>periodically]
D --> F{Valvular AFib?<br/>mech valve / mod-sev MS}
F -->|Yes| G[Warfarin<br/>INR 2-3]
F -->|No| H[DOAC preferred<br/>apixaban / rivaroxaban / edox / dabig]
A --> I[Rate vs Rhythm<br/>strategy]
I --> J[Rate Control<br/>BB or non-DHP CCB]
I --> K[Rhythm Control<br/>cardiovert + AAD<br/>or PVI ablation]Treatment
First-line
- Acute rate control (HR <110 at rest is reasonable target; <80 for symptomatic):
- • Beta-blocker (metoprolol, esmolol IV) — first-line
- • Non-dihydropyridine CCB (diltiazem, verapamil) — avoid if HFrEF
- • Digoxin — useful adjunct in HF or sedentary patients; slow onset
- Anticoagulation if CHA2DS2-VASc ≥2 (men) or ≥3 (women):
- • DOAC preferred (apixaban, rivaroxaban, edoxaban, dabigatran)
- • Warfarin required for mechanical valve or moderate-severe mitral stenosis ('valvular AFib')
- Rhythm vs rate: rate-control is non-inferior in most patients (AFFIRM), but early rhythm control may improve outcomes in newly diagnosed AFib (EAST-AFNET 4)
Second-line / adjunct
- Rhythm-control options:
- • Cardioversion (electrical or pharmacologic) if hemodynamically unstable, or with adequate anticoagulation
- • Antiarrhythmics: flecainide or propafenone (no structural heart disease); amiodarone (HF or CAD); sotalol, dofetilide
- • Catheter ablation (pulmonary vein isolation) — symptomatic paroxysmal AFib refractory to ≥1 antiarrhythmic, or first-line for symptomatic patients per recent guidelines
- Left atrial appendage occlusion (Watchman) for patients with stroke risk who cannot tolerate long-term anticoagulation
Complications
- Embolic stroke (5× increased risk; ~15% of all ischemic strokes are AFib-related)
- Tachycardia-induced cardiomyopathy from chronic rapid ventricular response
- Heart failure decompensation
- Anticoagulation-related bleeding
PANCE pearls
- CHA2DS2-VASc: CHF (1), HTN (1), Age ≥75 (2), Diabetes (1), Stroke/TIA history (2), Vascular disease (1), Age 65-74 (1), Sex (female) (1). Score ≥2 men or ≥3 women → anticoagulate.
- HAS-BLED estimates bleeding risk but does NOT exclude patients from anticoagulation — it identifies modifiable bleeding risk factors.
- Cardioversion safety: <48 h from onset → cardiovert without prior AC. >48 h or unknown → either TEE-guided or 3 weeks AC first. Always anticoagulate ≥4 weeks after cardioversion regardless.
- Wolf-Parkinson-White + AFib: AVOID AV-nodal blockers (BB, CCB, digoxin, adenosine) — can precipitate VF. Use procainamide or cardiovert.
- Holiday heart syndrome: AFib triggered by acute alcohol binge; usually self-terminates with abstinence and supportive care.
Images
References
- ACC/AHA/ACCP/HRS 2023 — 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation (Joglar et al., Circulation 2024)
- EAST-AFNET 4 — Early Rhythm-Control Therapy in Patients with Atrial Fibrillation (Kirchhof et al., NEJM 2020)
- AFFIRM — A Comparison of Rate Control and Rhythm Control in AFib (Wyse et al., NEJM 2002)
- CHA2DS2-VASc — Refining Clinical Risk Stratification for Stroke in AFib (Lip et al., Chest 2010)
- RE-LY / ARISTOTLE / ROCKET-AF — DOAC pivotal trials vs warfarin in AFib (Connolly NEJM 2009; Granger NEJM 2011; Patel NEJM 2011)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.