Premature Atrial and Ventricular Contractions
Common ectopic beats — usually benign in structurally normal hearts; high burden may herald cardiomyopathy and warrant evaluation.
Also known as: PAC, premature atrial contraction, premature atrial complex, PVC, premature ventricular contraction, ectopic beats
Overview
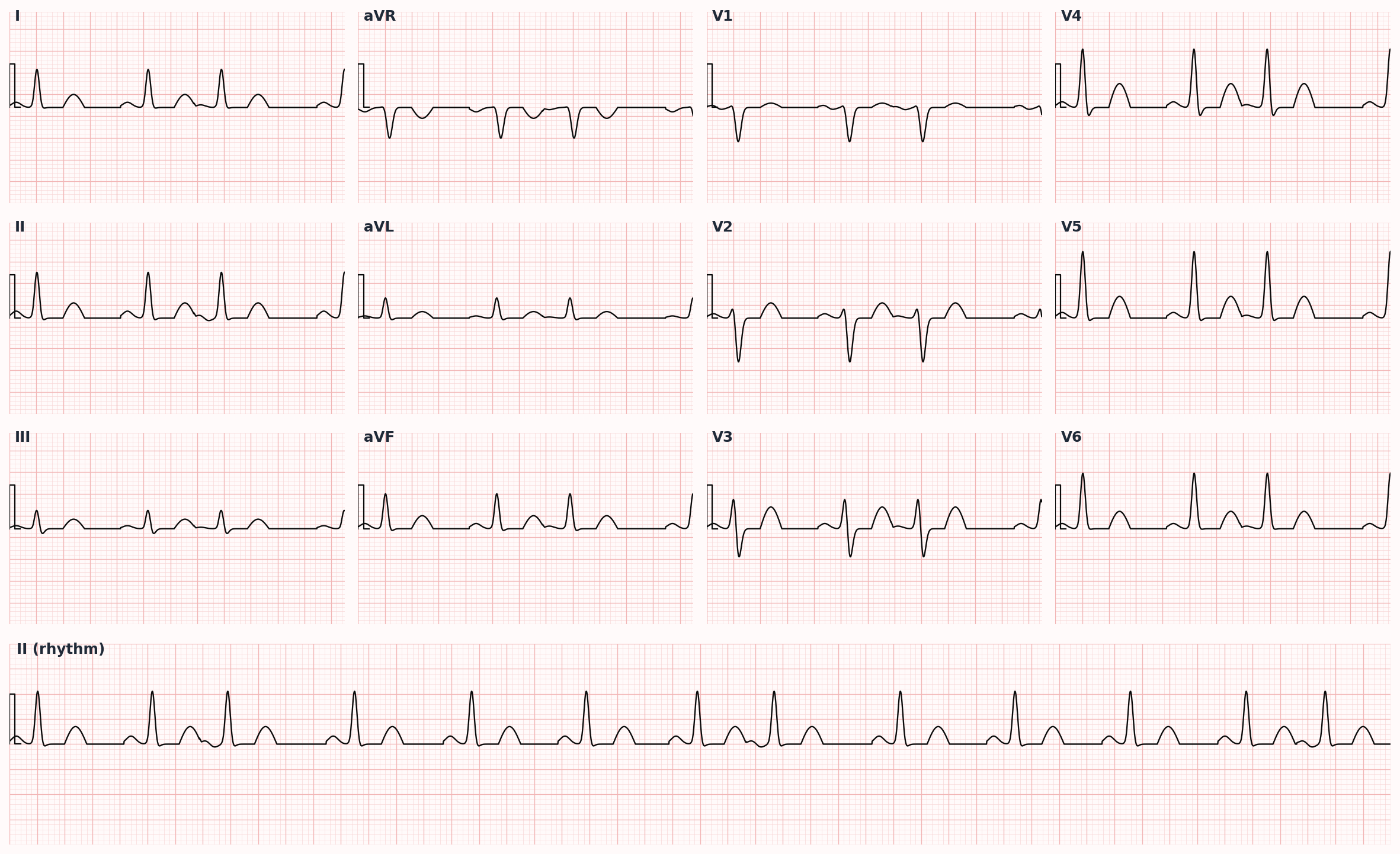
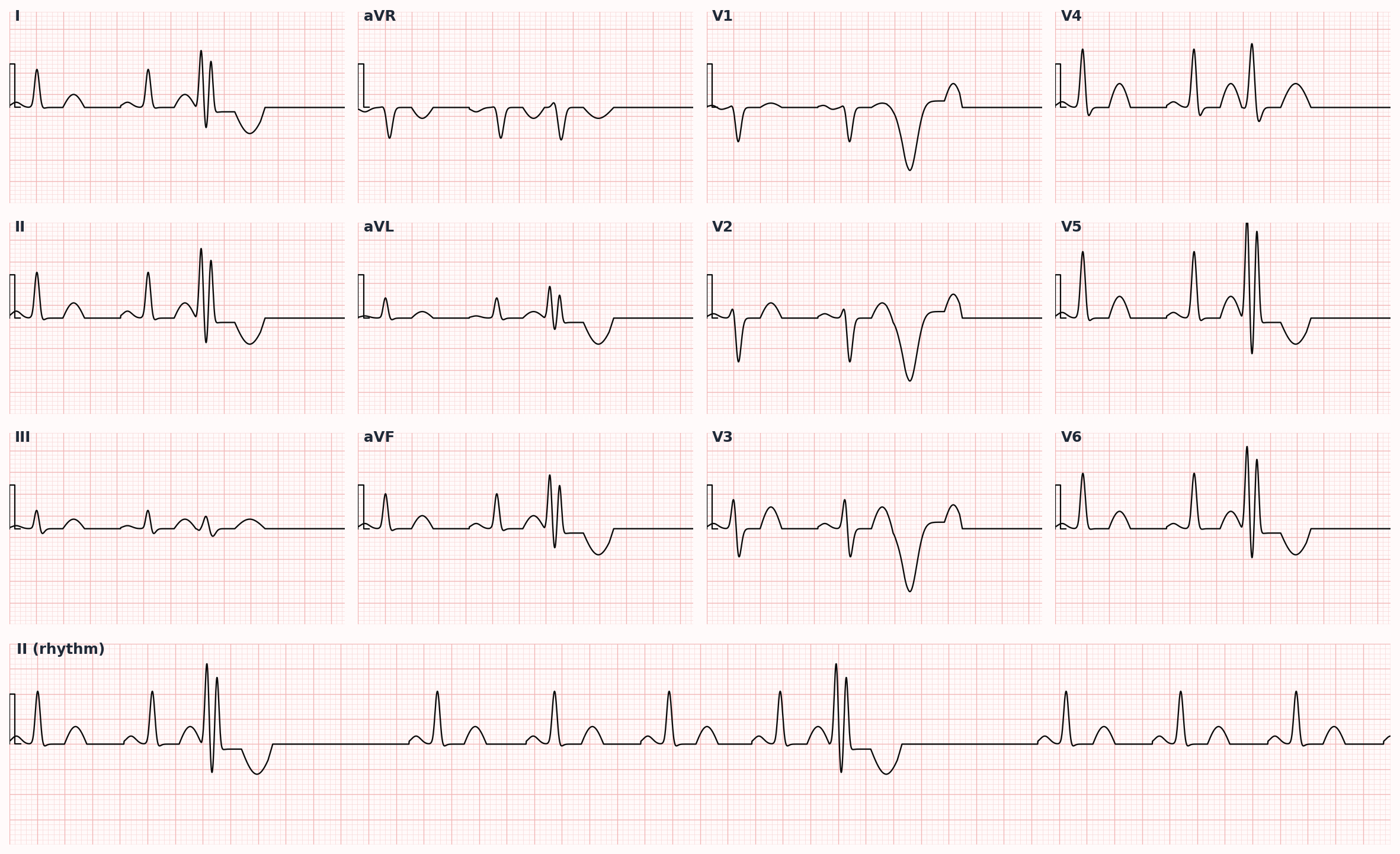
Premature atrial contractions (PACs) are early beats originating from ectopic foci within the atria, producing an early P wave (often with altered morphology) followed by a narrow QRS. Premature ventricular contractions (PVCs) originate below the AV node, generating a wide QRS (>120 ms) without a preceding P wave, often followed by a fully or partially compensatory pause. Both are common and often benign in structurally normal hearts.
Epidemiology
PACs and PVCs are extraordinarily common; >50% of healthy adults will have at least one PVC on ambulatory monitoring. Frequency rises with age and underlying cardiovascular disease. A PVC burden >10-15% of total beats on 24-hour Holter is associated with risk of PVC-induced cardiomyopathy.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Premature Atrial and Ventricular Contractions outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Caffeine, nicotine, alcohol, stimulants (cocaine, methamphetamine, decongestants), recreational drugs
- Electrolyte disturbances: hypokalemia, hypomagnesemia
- Hyperthyroidism
- Anemia, fever
- Anxiety, sympathetic activation, sleep deprivation
- Structural heart disease: prior MI, cardiomyopathy, valvular disease, heart failure
- Ischemia
- Sleep apnea
- Mitral valve prolapse
- Medications: digoxin (especially toxicity), bronchodilators (β-agonists, theophylline), QT-prolonging drugs
Pathophysiology
PACs arise from enhanced automaticity, triggered activity, or microreentry within atrial myocardium or pulmonary vein sleeves — the latter are a key substrate for atrial fibrillation. PVCs arise from similar mechanisms within ventricular tissue, most commonly the outflow tracts (especially the right ventricular outflow tract, producing a characteristic LBBB pattern with inferior axis) or fascicular Purkinje system. Frequent PVCs (>10-15% burden) can produce dyssynchronous ventricular contraction, ventricular remodeling, and a reversible cardiomyopathy.
Clinical presentation
Symptoms
- Often asymptomatic and found incidentally
- Palpitations described as 'skipped beats,' 'flip-flop,' or 'thump' (the strong post-extrasystolic beat is what patients often perceive)
- Lightheadedness, fatigue, or rarely syncope with very high burden
- Symptoms of heart failure if PVC-induced cardiomyopathy has developed
- Anxiety triggered by perceived irregular heartbeat
Signs / physical exam
- Irregular pulse with intermittent skipped or strong beats
- Variable intensity of S1 (with PVCs interrupting normal AV synchrony)
- Cannon A waves on JVP examination if AV dissociation
- Heart murmurs may vary in intensity beat-to-beat
- Otherwise normal exam unless underlying structural disease
Classic findings
PAC: early, narrow QRS preceded by an abnormal P wave, often followed by a non-compensatory pause. PVC: early, wide QRS without preceding P wave, often followed by a fully compensatory pause; the next sinus beat returns at the expected time.
Differential diagnosis
- Atrial fibrillation / atrial flutter (when frequent PACs in bigeminy) — Irregular rhythm without identifiable P waves vs PAC bigeminy with discrete early P; longer monitoring may clarify
- Sinus arrhythmia — Phasic variation in sinus rate with respiration; normal P wave morphology
- Ventricular tachycardia (when frequent PVCs/runs) — ≥3 consecutive PVCs at >100 bpm constitutes NSVT; sustained >30 sec is VT
- Aberrantly conducted PAC vs PVC — Preceding P wave (often abnormal) suggests PAC with aberrancy; AV dissociation/fusion beats favor PVC
- Pacemaker spikes — Distinguished by pacing artifact preceding QRS
- Catecholaminergic polymorphic VT (CPVT) — Exercise- or emotion-triggered bidirectional VT in young patients with normal resting ECG; RYR2 mutations
- Arrhythmogenic right ventricular cardiomyopathy (ARVC) — LBBB-pattern PVCs with epsilon waves, T-wave inversion V1-V3; RV structural abnormalities on MRI
Diagnostic workup
Labs
- BMP including potassium, magnesium
- TSH
- CBC for anemia
- Troponin if ischemia suspected
Imaging
- 12-lead ECG to characterize morphology and define PVC origin (RVOT, LVOT, fascicular, etc.)
- Ambulatory 24-48 hour Holter monitor to quantify burden — key for risk stratification and need for further workup; PVC burden >10-15% suggests need for further evaluation
- Echocardiography in symptomatic patients, those with frequent PVCs (>5-10%), or any suspicion of structural heart disease
- Stress testing if symptoms are exertional or to assess suppression vs provocation with exercise
- Cardiac MRI for unusual morphology, suspected ARVC, sarcoid, or unexplained cardiomyopathy
- Electrophysiology study selectively in patients considered for catheter ablation
Diagnostic algorithm
| Feature | PAC | PVC |
|---|---|---|
| P wave before QRS | Yes (early, often abnormal morphology) | No |
| QRS width | Narrow (<120 ms) unless aberrancy | Wide (≥120 ms) |
| Post-extrasystolic pause | Non-compensatory (resets sinus node) | Fully compensatory (sinus node not reset) |
| Common origin | Atrial myocardium, pulmonary veins | RVOT, fascicular system, LVOT, scar |
| Risk if high burden | Initiation of AFib | PVC-induced cardiomyopathy |
| First-line therapy if symptomatic | Beta-blocker, trigger modification | Beta-blocker, trigger modification |
| Definitive therapy (refractory) | Pulmonary vein ablation (if triggering AFib) | Catheter ablation (especially RVOT) |
Treatment
First-line
- Asymptomatic PACs/PVCs with structurally normal heart and low burden: reassurance and observation — these are typically benign
- Address modifiable triggers: reduce caffeine, alcohol, stimulant use, nicotine; correct electrolyte abnormalities; treat hyperthyroidism, anemia, sleep apnea; minimize stress; ensure adequate sleep
- Beta-blockers (metoprolol, propranolol, atenolol) — first-line pharmacologic therapy for symptomatic PACs or PVCs; nondihydropyridine CCBs (diltiazem, verapamil) are alternatives, particularly for idiopathic RVOT or fascicular PVCs
Second-line / adjunct
- Class IC antiarrhythmics (flecainide, propafenone) for symptomatic PVCs in structurally normal hearts (avoid in CAD, LV dysfunction)
- Amiodarone for symptomatic PVCs in patients with structural heart disease or HF, though chronic toxicity profile limits enthusiasm
- Catheter ablation for: symptomatic PVCs refractory to medical therapy, PVC-induced cardiomyopathy (high burden + reduced EF), or specific high-yield morphologies (RVOT PVCs have ~90% ablation success)
- Treat underlying structural heart disease, ischemia, or HF aggressively
- ICD is NOT indicated for PVCs alone in the absence of high-risk markers (sustained VT, low EF meeting primary prevention criteria, etc.)
Complications
- PVC-induced cardiomyopathy (typically with >10-15% burden, often reversible with PVC suppression or ablation)
- Triggering of sustained ventricular tachyarrhythmias in patients with structural heart disease
- Initiation of atrial fibrillation by frequent PACs (especially those originating in pulmonary veins)
- Anxiety, depression, reduced quality of life from symptom burden
- Inappropriate or unnecessary cardiac testing
PANCE pearls
- PVC-induced cardiomyopathy: typically requires burden >10-15% of total beats on 24-hour monitoring. EF often improves substantially after suppression with medication or ablation — the cardiomyopathy is reversible.
- Right ventricular outflow tract (RVOT) PVCs (LBBB morphology, inferior axis, transition V3-V4) are the most common idiopathic PVCs in structurally normal hearts and respond well to catheter ablation.
- PACs originating in pulmonary veins are the dominant trigger for AFib initiation — frequent PACs can be a harbinger.
- Compensatory pause: PVCs typically have a FULLY compensatory pause (the next sinus beat returns at expected time because the PVC does not reset the sinus node); PACs typically have an INCOMPLETE compensatory pause (resetting the sinus node).
- Cardiac MRI is useful when PVC morphology suggests ARVC, sarcoidosis, or other structural substrate not seen on echo.
Images
References
- AHA/ACC/HRS 2017 — 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death (Al-Khatib et al., JACC 2018)
- EHRA/HRS/APHRS 2019 — EHRA/HRS/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias (Cronin et al., Heart Rhythm 2020)
- AHA Statement 2020 — Premature Ventricular Contractions and Their Role in the Development of Cardiomyopathy: AHA Scientific Statement (Marcus, Circulation 2020)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.