Acute Pericarditis
Inflammation of the pericardium — pleuritic chest pain improved by leaning forward, friction rub, diffuse ST elevation with PR depression.
Also known as: acute pericarditis, pericarditis, viral pericarditis
Overview
Inflammation of the pericardial sac with or without pericardial effusion, defined by at least 2 of: characteristic chest pain, pericardial friction rub, new widespread ST elevation or PR depression on ECG, or new/worsening pericardial effusion.
Epidemiology
Accounts for ~5% of ED chest pain visits with non-ischemic etiology. Most often idiopathic or viral; men 20-50 years most commonly affected.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Acute Pericarditis outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Recent viral illness (coxsackievirus, echovirus, adenovirus, EBV, influenza, SARS-CoV-2)
- Post-myocardial infarction (early peri-infarction pericarditis or late Dressler syndrome)
- Recent cardiac surgery or PCI (post-cardiotomy syndrome)
- Autoimmune disease: SLE, rheumatoid arthritis, scleroderma
- Uremia (in undialyzed or under-dialyzed CKD)
- Malignancy (lung, breast, lymphoma; metastatic spread)
- Tuberculosis (most common cause worldwide in endemic regions)
- Radiation therapy, certain drugs (hydralazine, procainamide, isoniazid)
Pathophysiology
Inflammation of the visceral and parietal pericardium produces increased capillary permeability, fibrin deposition, and exudate. The roughened layers generate friction rub. Sympathetic involvement of the diaphragm (phrenic nerve) causes referred shoulder/trapezius pain. Inflammation may extend to the epicardium (myopericarditis) or produce significant effusion.
Clinical presentation
Symptoms
- Sharp, pleuritic, retrosternal or left precordial chest pain
- Worse supine, better leaning forward
- Radiation to trapezius ridge (highly specific — phrenic nerve)
- Low-grade fever, dyspnea, fatigue
- Antecedent viral prodrome (URI, GI symptoms) common
Signs / physical exam
- Pericardial friction rub — three-component, scratchy, best at LLSB with patient leaning forward
- Tachycardia
- Low-grade fever
- Signs of effusion (muffled heart sounds, Beck triad) if progressing to tamponade
Differential diagnosis
- Acute coronary syndrome / STEMI — Regional (not diffuse) ST elevation with reciprocal changes; high troponin; risk factor profile
- Pulmonary embolism — Pleuritic pain with dyspnea and hypoxia; S1Q3T3, right heart strain; D-dimer / CTPA
- Aortic dissection — Tearing back-radiating pain, pulse deficit, widened mediastinum on CXR
- Pneumonia / pleurisy — Fever with productive cough, focal lung findings, infiltrate on CXR
- Early repolarization variant — ST elevation on ECG in young men WITHOUT PR depression or evolution; benign
- Myocarditis / myopericarditis — Pericarditis features + elevated troponin and possibly LV dysfunction
- Costochondritis — Reproducible chest wall tenderness, no rub, normal ECG
Diagnostic workup
Diagnostic criteria
Acute pericarditis ≥2 of 4: (1) sharp pleuritic pain improved leaning forward, (2) pericardial friction rub, (3) new widespread ST elevation or PR depression, (4) new/worsening pericardial effusion. Supporting features: elevated CRP, evidence of inflammation on imaging.
Labs
- Troponin — modest elevation suggests myopericarditis; high values warrant additional workup
- CBC, CRP, ESR (elevated CRP supports diagnosis and guides response to therapy)
- BMP, BUN/Cr (uremic etiology)
- ANA, RF, TSH if autoimmune cause suspected; HIV and TB testing in appropriate populations
- Blood cultures if febrile and effusion present
Imaging
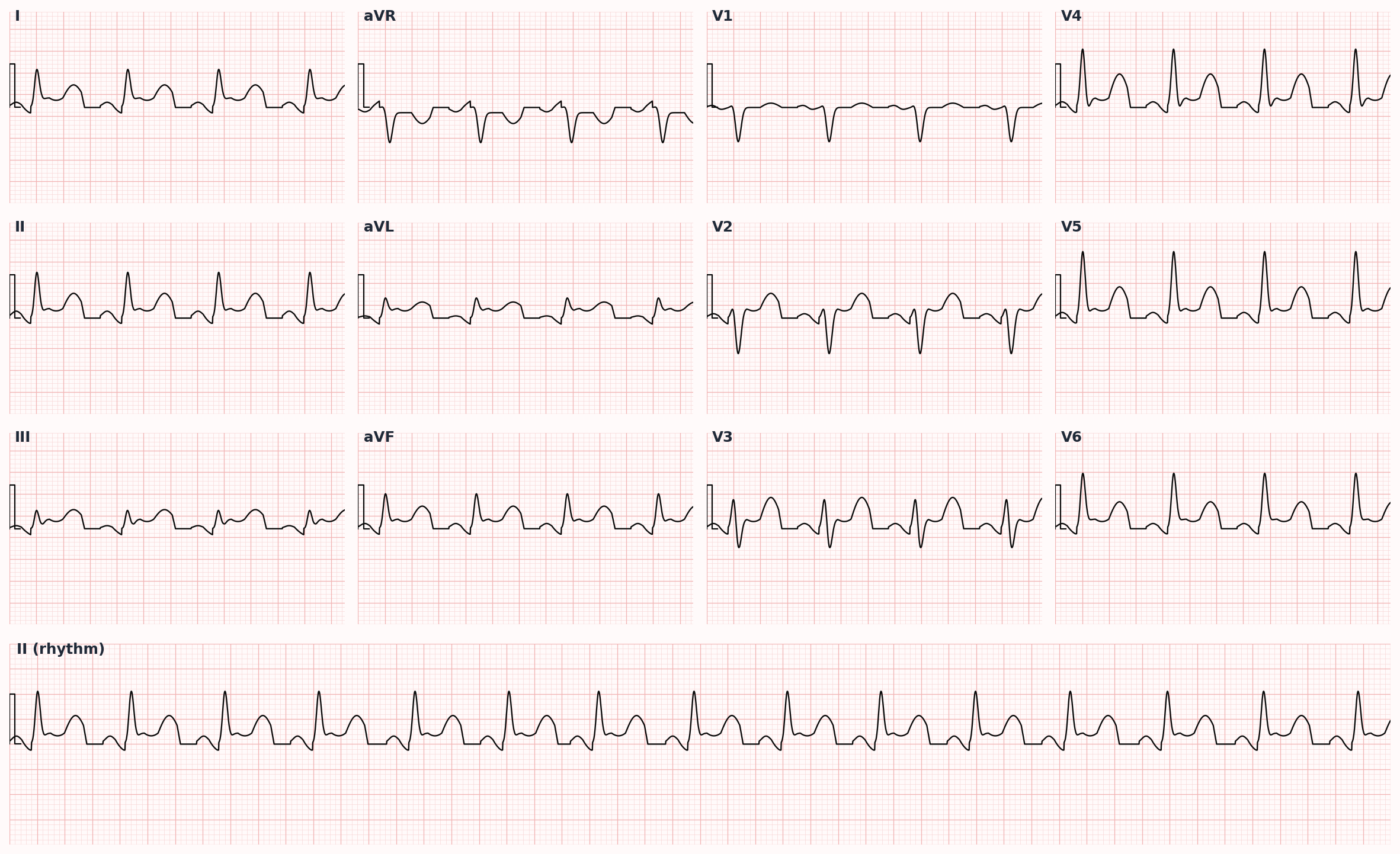
- 12-lead ECG — diffuse concave ST elevation with PR segment depression (PR elevation in aVR is reciprocal — early sign)
- Echocardiography — assess for pericardial effusion and ventricular function (rule out tamponade and myocarditis)
- CXR — typically normal; cardiomegaly only with large effusion
- Cardiac MRI — late gadolinium enhancement of pericardium; useful for myopericarditis or recurrent disease
- Chest CT for suspected purulent or constrictive disease
Diagnostic algorithm
| Feature | Pericarditis | STEMI | Early repolarization |
|---|---|---|---|
| ST elevation distribution | Diffuse, concave | Regional, convex | Often precordial |
| PR depression | Present (PR elevation in aVR) | Absent | Absent |
| Reciprocal ST depression | Absent (except aVR, V1) | Present | Absent |
| Q waves | Absent | May develop | Absent |
| Troponin | Normal or mildly elevated | Markedly elevated | Normal |
| Evolution | Diffuse ST resolves over days then T inversion | ST resolves, Q waves and T inversion form | Stable over time |
Treatment
First-line
- NSAIDs — ibuprofen 600-800 mg PO TID × 1-2 weeks then taper, OR aspirin 750-1000 mg PO TID (preferred post-MI pericarditis)
- Colchicine 0.5 mg PO BID (0.5 mg daily if <70 kg) × 3 months — added to NSAID for FIRST episode reduces recurrence (COPE / ICAP trials)
- Proton pump inhibitor while on high-dose NSAIDs
- Activity restriction until symptoms resolve and CRP normalizes (≥3 months for athletes with myopericarditis)
- Treat underlying cause: dialysis for uremia, antimicrobials for purulent, TB therapy if confirmed
Second-line / adjunct
- Corticosteroids (prednisone 0.25-0.5 mg/kg/day with slow taper) — reserved for NSAID/colchicine failure, contraindication, or specific etiologies (autoimmune, uremic) — increases recurrence risk in idiopathic disease
- Add colchicine to recurrent pericarditis × 6 months (CORE / CORP trials)
- Refractory recurrent pericarditis — IL-1 inhibitors (anakinra, rilonacept; RHAPSODY trial); IVIG; azathioprine
- Pericardiectomy for refractory recurrent or constrictive disease
Complications
- Pericardial effusion → cardiac tamponade
- Recurrent pericarditis (15-30% after first episode)
- Chronic constrictive pericarditis
- Myopericarditis with LV dysfunction
- Purulent pericarditis with abscess formation
PANCE pearls
- Diffuse concave ST elevation with PR depression — PR elevation in aVR is an early specific sign.
- Adding colchicine to NSAIDs at first presentation cuts recurrence roughly in half.
- Corticosteroids worsen recurrence in idiopathic pericarditis — reserve for autoimmune or NSAID failure.
- Trapezius ridge pain is highly specific for pericardial irritation (phrenic referral).
- Pericarditis post-MI: early (peri-infarction, days 1-3) is common; Dressler syndrome (2-10 weeks) is now rare in the reperfusion era.
Images
References
- ESC 2015 — 2015 ESC Guidelines for the Diagnosis and Management of Pericardial Diseases (Adler et al., Eur Heart J 2015)
- ICAP Trial — Colchicine for Acute Pericarditis (Imazio et al., NEJM 2013)
- CORP Trial — Colchicine for Recurrent Pericarditis (Imazio et al., Ann Intern Med 2011)
- RHAPSODY Trial — Rilonacept for Recurrent Pericarditis (Klein et al., NEJM 2021)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.