Supraventricular Tachycardia (AVNRT / AVRT)
Regular narrow-complex tachycardia from reentry involving AV node ± accessory pathway — vagal maneuvers, adenosine, ablation.
Also known as: SVT, AVNRT, AVRT, PSVT, paroxysmal supraventricular tachycardia, WPW, Wolff-Parkinson-White
Overview
Paroxysmal supraventricular tachycardia (PSVT) is a regular narrow-complex tachycardia originating above the bundle of His. Two main reentrant mechanisms: AV nodal reentrant tachycardia (AVNRT) uses dual AV nodal pathways; AV reentrant tachycardia (AVRT) uses an accessory pathway (e.g., Wolff-Parkinson-White).
Epidemiology
AVNRT is most common SVT in adults (~60%), female predominance, often presents 20s-40s. AVRT (WPW) accounts for ~30%, often presents in younger patients (teens-30s) and is male-predominant.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Supraventricular Tachycardia (AVNRT / AVRT) outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- AVNRT: most often no structural heart disease; female sex; triggers include stress, caffeine, alcohol, stimulants
- AVRT: accessory pathway is congenital; WPW prevalence ~1-3 per 1000
- Associations: Ebstein anomaly (right-sided pathways), hypertrophic cardiomyopathy
- Hyperthyroidism, fever, dehydration, stimulant use as triggers
Pathophysiology
AVNRT: dual AV nodal pathways (slow + fast) create a microreentry circuit confined to the AV node. Typical (slow-fast) form — antegrade slow, retrograde fast — has retrograde P waves buried in or just after the QRS. AVRT: macroreentry involves AV node and an accessory pathway. Orthodromic AVRT (antegrade through AV node, retrograde through accessory) is narrow QRS; antidromic AVRT (antegrade through accessory, retrograde through AV node) is wide QRS.
Clinical presentation
Symptoms
- Sudden-onset palpitations with abrupt termination
- Lightheadedness, dyspnea, anxiety
- Chest pressure, near-syncope or syncope
- Polyuria after episode (atrial natriuretic peptide release)
- Pre-existing WPW: may present with palpitations or rarely sudden death from pre-excited atrial fibrillation degenerating to VF
Signs / physical exam
- Regular rapid pulse 150-220 bpm
- Frog sign / cannon A waves in AVNRT (simultaneous atrial and ventricular contraction)
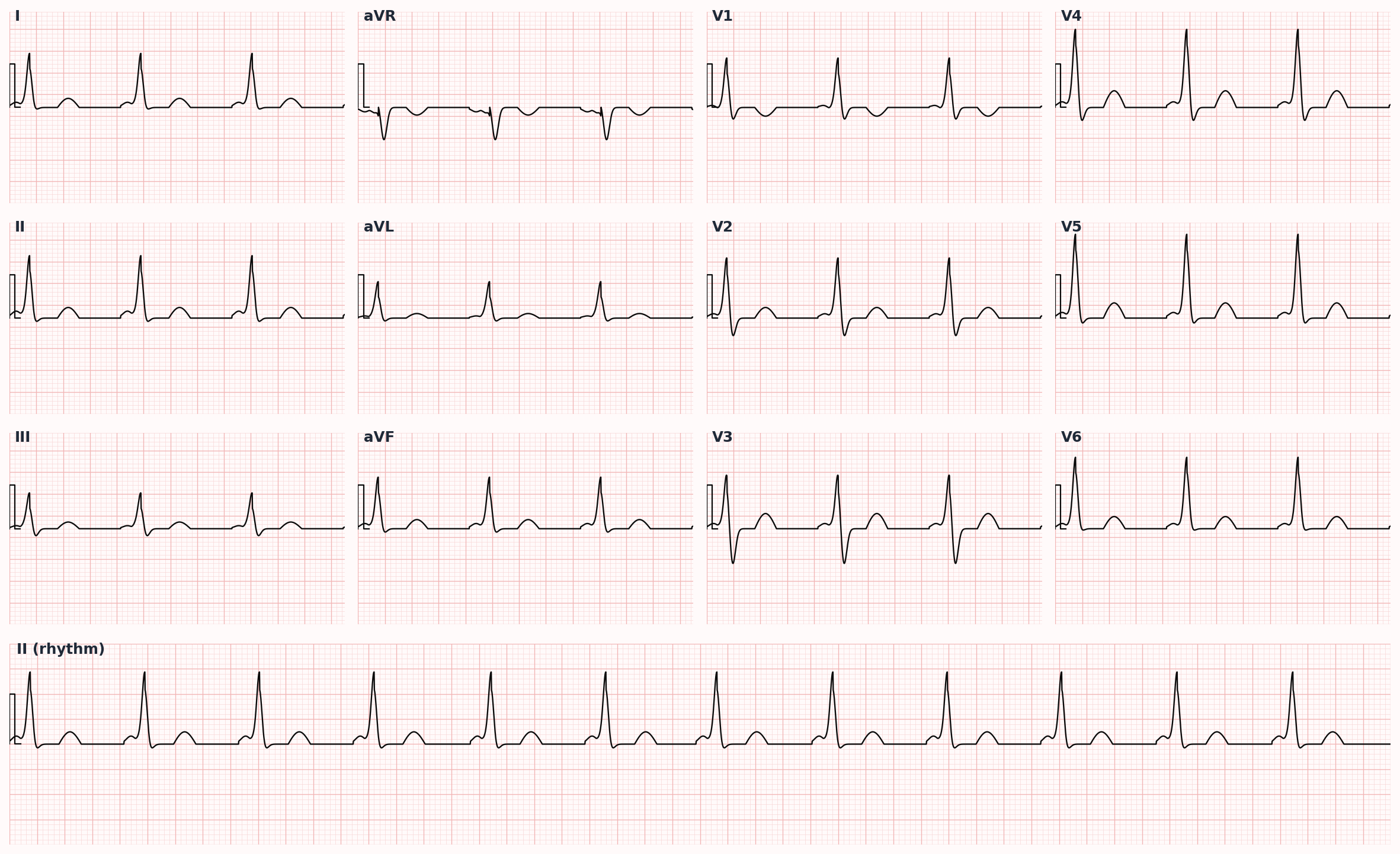
- Sinus rhythm: short PR (<120 ms) and delta wave (slurred upstroke of QRS) in manifest WPW
Differential diagnosis
- Sinus tachycardia — Rate <160, P waves identical to sinus, gradual onset/offset, identifiable trigger (fever, anemia, hypovolemia)
- Atrial fibrillation — Irregularly irregular without discrete P waves
- Atrial flutter — Sawtooth flutter waves, ventricular response often 150 from 2:1 conduction; consider flutter in any HR 150
- Atrial tachycardia — P-wave morphology different from sinus, may be incessant
- Multifocal atrial tachycardia — ≥3 P-wave morphologies in patient with COPD
- Junctional tachycardia — Narrow QRS without distinct P waves; rare in adults outside of post-cardiac surgery and digoxin toxicity
- VT or SVT with aberrancy — Wide QRS — see VT entry for distinguishing features
Diagnostic workup
Diagnostic criteria
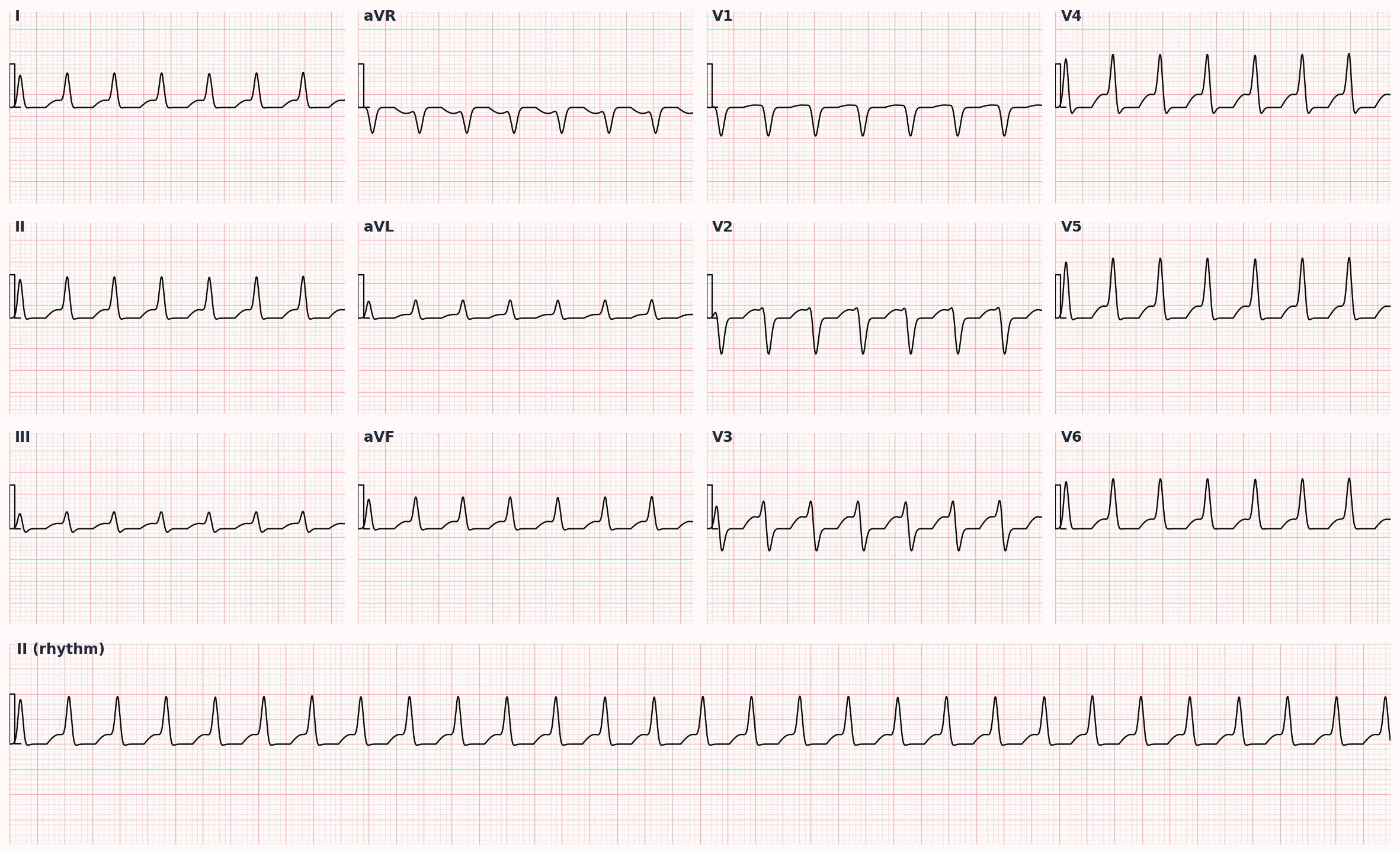
Typical AVNRT: rate 150-250, narrow QRS, retrograde P waves not visible or just after QRS as pseudo-R' in V1 / pseudo-S in inferior leads. Orthodromic AVRT: retrograde P visible after QRS in ST segment. Manifest WPW on resting ECG: PR <120 ms + delta wave + wide QRS + secondary ST-T changes.
Labs
- Electrolytes, magnesium, TSH
- CBC if anemia suspected as trigger
- Troponin if associated chest pain
Imaging
- 12-lead ECG during tachycardia and in sinus rhythm
- Echocardiogram to assess for structural disease, especially before ablation
- Holter or event monitor for diagnosis if episodes are infrequent
- Electrophysiology study — diagnostic and therapeutic (ablation)
Diagnostic algorithm
flowchart TD
A[Regular narrow-complex<br/>tachycardia 150-220 bpm] --> B{Hemodynamically<br/>stable?}
B -->|No| C[Synchronized<br/>cardioversion 50-100 J]
B -->|Yes| D[Vagal maneuvers<br/>modified Valsalva]
D --> E{Converted?}
E -->|No| F[Adenosine 6 mg<br/>then 12 mg × 2]
E -->|Yes| G[Identify SVT type<br/>on 12-lead]
F --> H{Converted?}
H -->|No| I[IV diltiazem or<br/>metoprolol]
H -->|Yes| G
G --> J{Recurrent or<br/>symptomatic?}
J -->|Yes| K[Catheter ablation<br/>>95% cure for AVNRT/AVRT]
J -->|No| L[Reassurance, vagal<br/>maneuvers PRN]Treatment
First-line
- Stable narrow-complex SVT: vagal maneuvers first — Valsalva (modified REVERT maneuver — supine with leg lift improves success), carotid sinus massage (avoid bilateral or in patients with carotid bruits or recent TIA)
- Adenosine 6 mg rapid IV push followed by saline flush; if no conversion in 1-2 min, give 12 mg, then repeat 12 mg — warn the patient about transient chest pressure and asystole
- If adenosine fails or is contraindicated: IV diltiazem 0.25 mg/kg over 2 min OR IV metoprolol 5 mg over 2 min × up to 3 doses
- Synchronized cardioversion 50-100 J biphasic for hemodynamic instability
- For PRE-EXCITED atrial fibrillation (irregularly irregular WIDE complex in WPW): IV procainamide 20-50 mg/min OR ibutilide; AVOID adenosine, AV nodal blockers, and digoxin (can accelerate accessory pathway to VF)
Second-line / adjunct
- Long-term: beta-blockers (metoprolol, atenolol), non-dihydropyridine CCBs (diltiazem, verapamil), or flecainide/propafenone (only if no structural disease)
- Catheter ablation — first-line option for symptomatic recurrent SVT; >95% success for typical AVNRT (slow pathway modification) and AVRT (accessory pathway ablation)
- Patient education on Valsalva for self-termination
- Asymptomatic WPW: risk stratification with exercise testing and EP study — ablation if accessory pathway has short antegrade refractory period
Complications
- Hemodynamic compromise during sustained tachycardia
- Tachycardia-mediated cardiomyopathy with persistent or frequent arrhythmia
- WPW: pre-excited atrial fibrillation degenerating to ventricular fibrillation (rare but dreaded)
- Ablation complications: AV block (typical AVNRT ablation), cardiac tamponade, vascular access, stroke (left-sided ablation)
PANCE pearls
- Adenosine has a half-life of ~10 seconds — must push fast and flush; warn patient about chest pressure and impending doom feeling.
- AVOID adenosine and all AV nodal blockers in pre-excited atrial fibrillation (WPW + irregular wide complex) — use procainamide or DC cardioversion.
- AVNRT pseudo-R' in V1 and pseudo-S in inferior leads compared to sinus rhythm tracing is highly suggestive.
- Modified Valsalva (REVERT trial — passive leg raise after strain) converts >40% of SVT vs ~17% with standard Valsalva.
- Catheter ablation is curative for AVNRT and AVRT and is offered as first-line for any recurrent or symptomatic case.
Images
References
- ACC/AHA/HRS 2015 SVT — 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia (Page et al., Circulation 2016)
- ESC 2019 SVT — 2019 ESC Guidelines for the Management of Patients with Supraventricular Tachycardia (Brugada et al., Eur Heart J 2020)
- REVERT Trial — Postural Modification to the Standard Valsalva Manoeuvre for Emergency Treatment of Supraventricular Tachycardias (Appelboam et al., Lancet 2015)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.