Atrioventricular (AV) Blocks
Delay or failure of AV nodal or infranodal conduction — first-degree, Mobitz I/II, third-degree (complete).
Also known as: AV block, heart block, first-degree AV block, Mobitz I, Wenckebach, Mobitz II, third-degree heart block, complete heart block
Overview
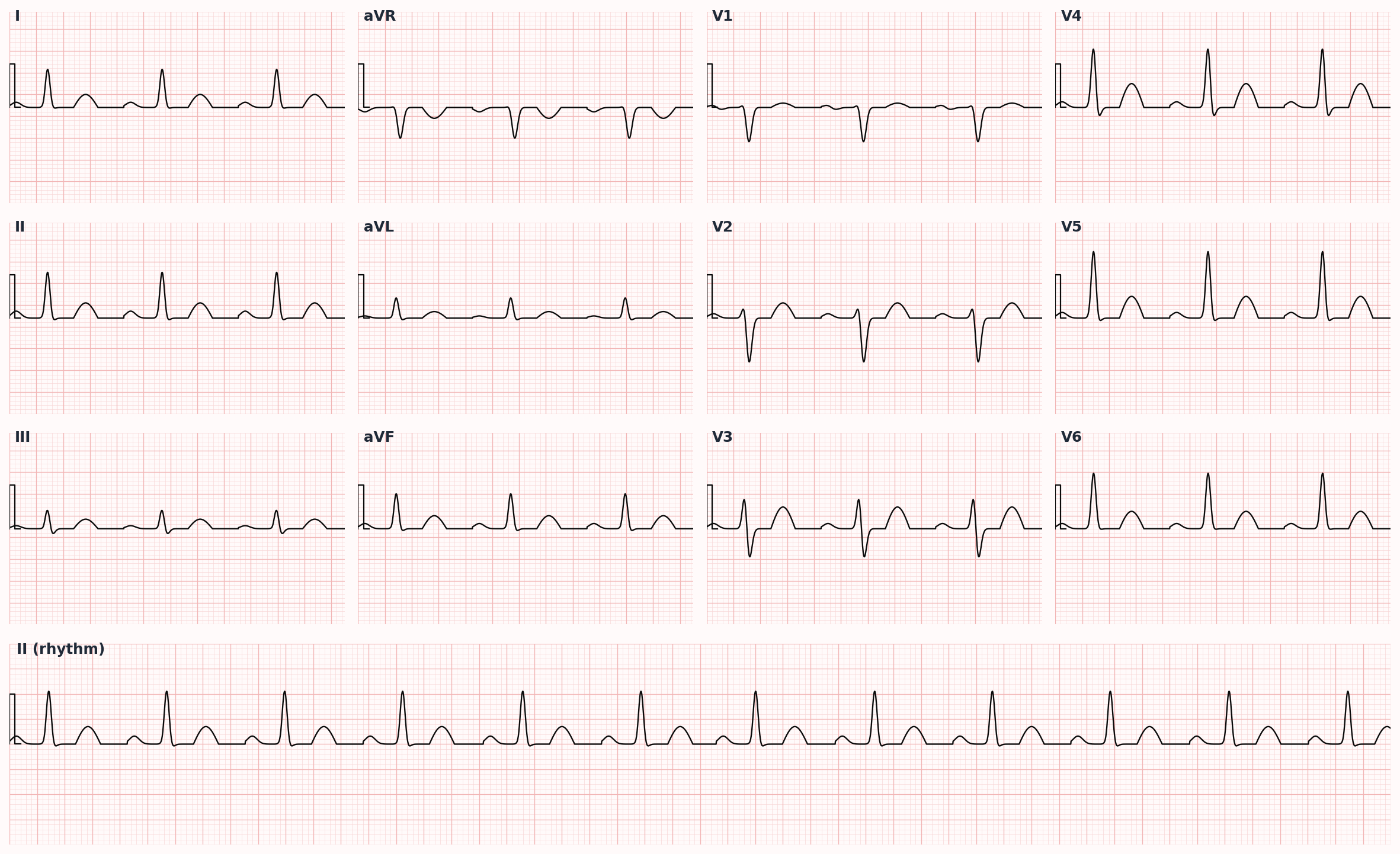
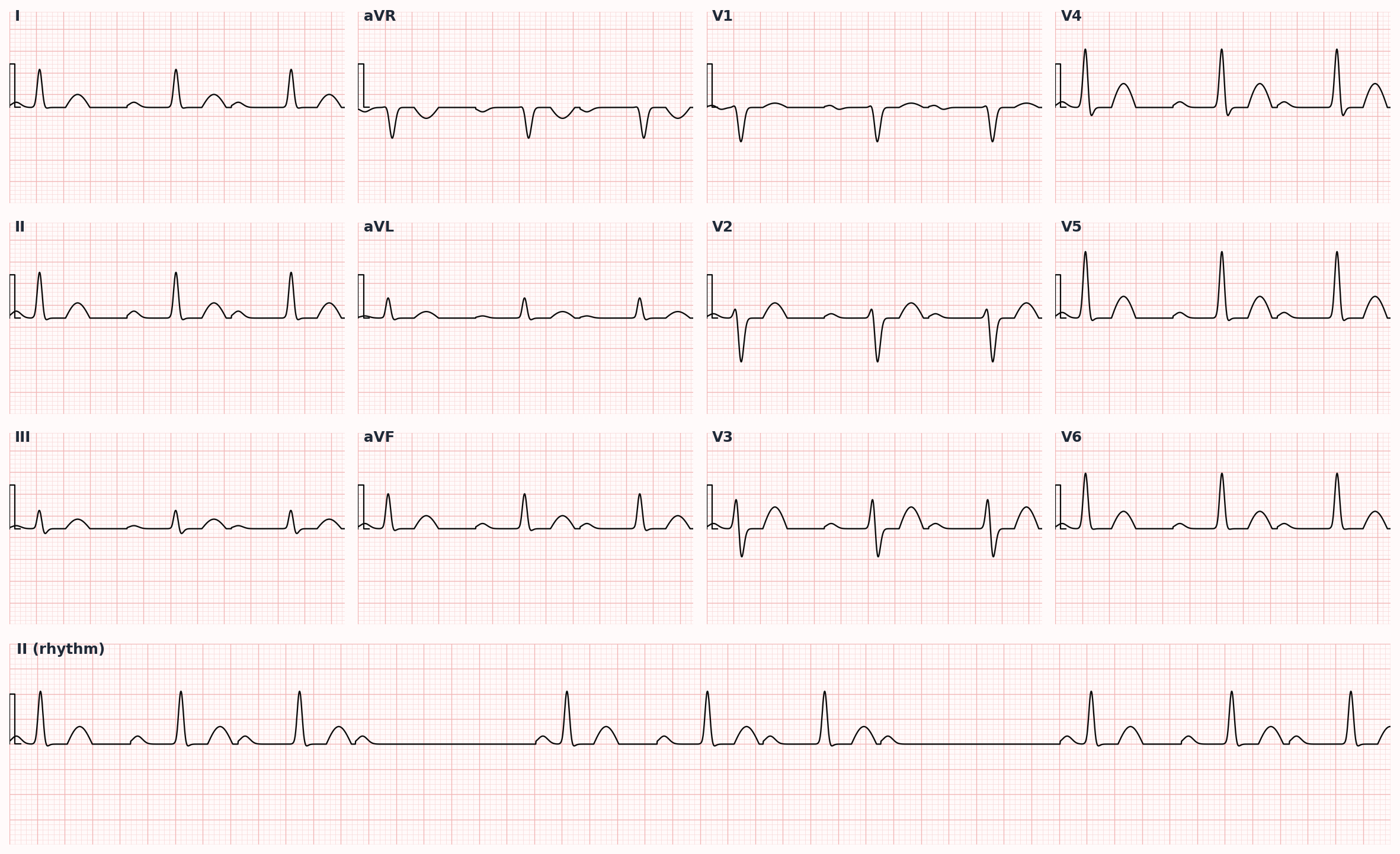
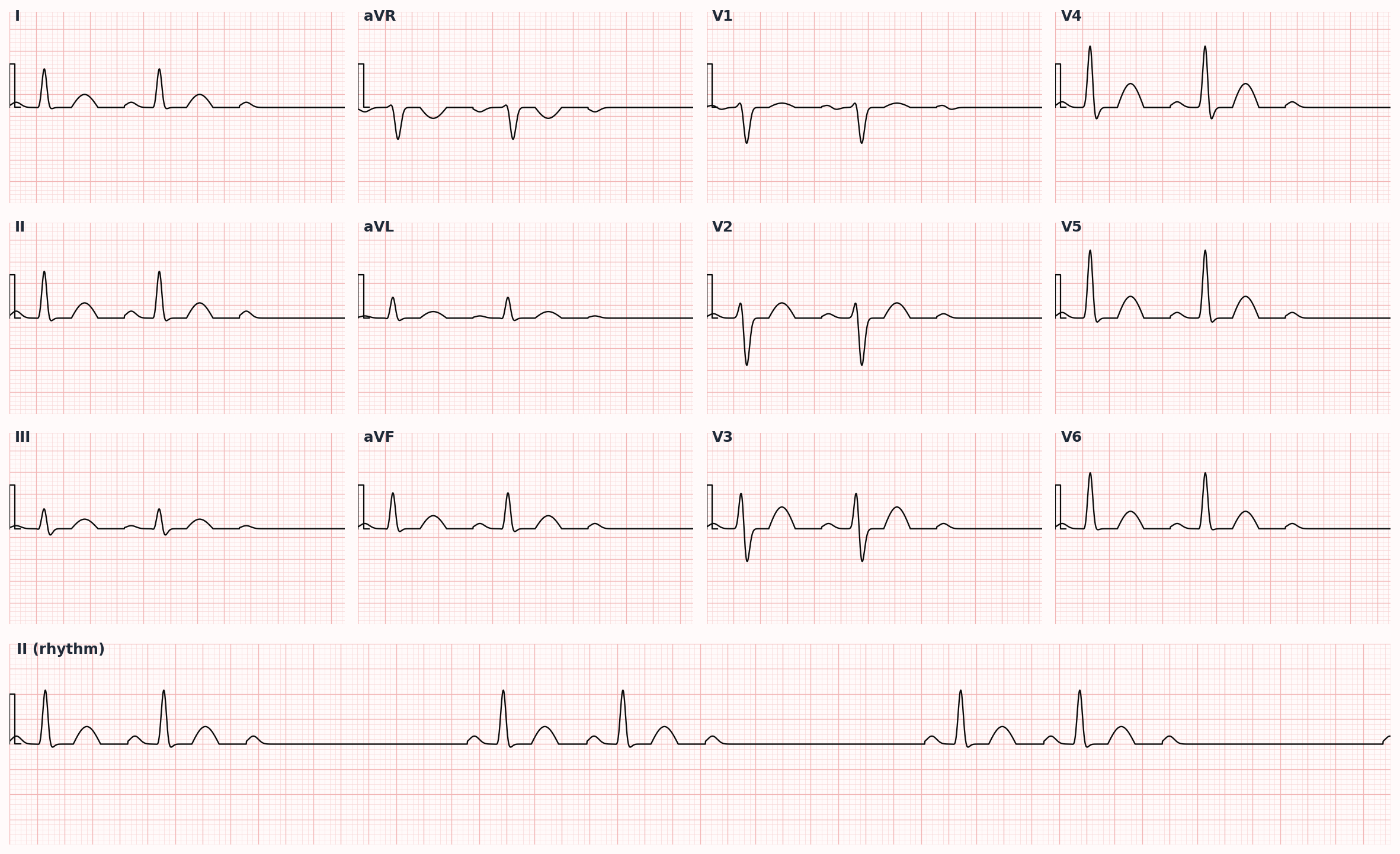
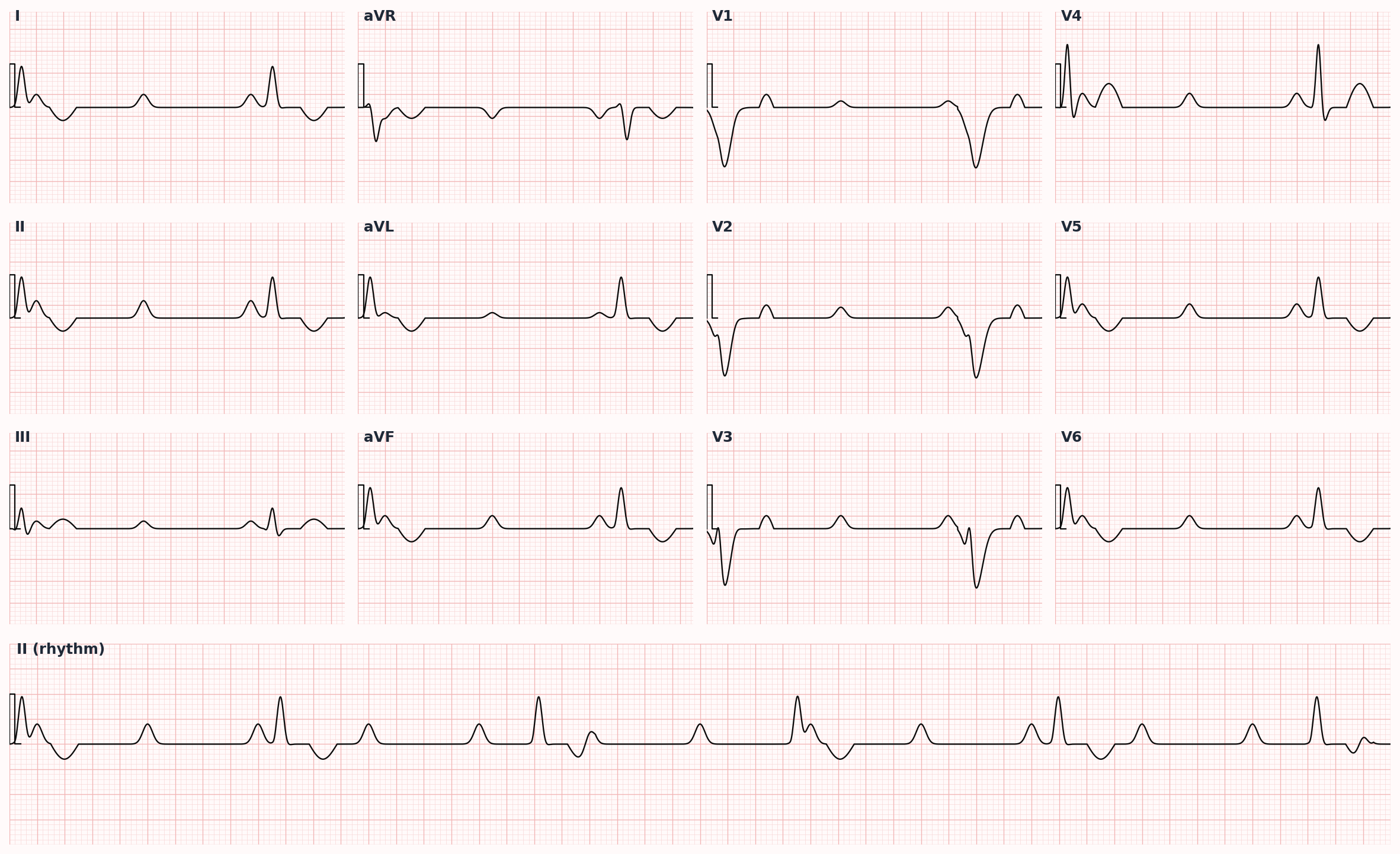
Disorders of conduction between atria and ventricles. First-degree: PR >200 ms with 1:1 conduction. Second-degree Mobitz I (Wenckebach): progressive PR prolongation until a non-conducted P wave. Mobitz II: constant PR with intermittent dropped beats. Third-degree (complete): AV dissociation with independent atrial and ventricular rates.
Epidemiology
Prevalence rises sharply with age and structural heart disease. Mobitz II and third-degree blocks reflect infranodal disease and are far more likely to progress to symptomatic or fatal bradycardia than nodal blocks.
Keep reading — start your free trial
You've read your 2 free diagnosis previews. Create your free account to unlock the full Atrioventricular (AV) Blocks outline — plus all 514 diagnoses, 5,500+ board-style questions, flashcards, and an AI tutor. Your 7-day free trial includes everything, and there's no credit card required.
Risk factors
- Age-related conduction system degeneration (Lev and Lenègre disease)
- Ischemic heart disease, especially inferior MI (transient AV nodal block) and anterior MI (infranodal block)
- Medications: beta-blockers, non-dihydropyridine CCBs (diltiazem, verapamil), digoxin, amiodarone, ivabradine, clonidine
- Increased vagal tone (athletes, sleep, carotid sinus hypersensitivity)
- Cardiomyopathies and infiltrative diseases: amyloidosis, sarcoidosis, hemochromatosis
- Lyme carditis, endocarditis with abscess, rheumatic fever
- Iatrogenic: post-cardiac surgery (especially aortic/mitral surgery, TAVR), catheter ablation
- Congenital complete heart block (maternal anti-Ro/SSA antibodies)
Pathophysiology
Conduction can fail in the AV node (typically Wenckebach — vagal influence, drug effect, ischemia from RCA territory) or in the His-Purkinje system below (Mobitz II and most complete blocks — fibrotic or ischemic). Nodal blocks are usually benign and responsive to atropine; infranodal blocks generally are not.
Clinical presentation
Symptoms
- First-degree and Mobitz I: usually asymptomatic, incidental finding
- Mobitz II and third-degree: fatigue, dyspnea, presyncope, syncope (Stokes-Adams attack), heart failure, angina
- Worsening with negative chronotropic medications
Signs / physical exam
- Bradycardia
- Cannon A waves in third-degree block (atrial contraction against closed tricuspid valve)
- Variable S1 intensity in third-degree block (AV dissociation)
- Wide pulse pressure in complete heart block (large stroke volume)
- Signs of heart failure in chronic high-grade block
Differential diagnosis
- Sinus bradycardia — Slow but 1:1 conduction with normal PR; no dropped beats
- Blocked premature atrial complex — Non-conducted P wave but P morphology differs from sinus and timing is premature
- Vagally mediated AV block — Often nocturnal, asymptomatic, athletes; responds to exercise; benign
- Junctional escape rhythm — Narrow QRS 40-60 bpm with no P or inverted retrograde P; backup rhythm in sinus arrest or complete block
- Ventricular escape rhythm — Wide QRS 20-40 bpm; backup in complete heart block with infranodal disease
- Atrial fibrillation with regularized slow ventricular rate — Suggests complete AV block with junctional/ventricular escape
Diagnostic workup
Diagnostic criteria
First-degree: PR interval >200 ms with each P followed by a QRS. Mobitz I: progressive PR prolongation, then a single dropped QRS; cycle repeats. Mobitz II: constant PR, sudden dropped QRS without prior PR change. Third-degree: complete AV dissociation, atrial rate exceeds ventricular rate, ventricular escape rhythm (junctional 40-60 narrow, or ventricular 20-40 wide).
Labs
- BMP, magnesium, calcium, TSH
- Troponin if ischemic etiology suspected
- Digoxin level if applicable
- Lyme serology, sarcoidosis workup in selected patients
Imaging
- 12-lead ECG — diagnostic; characterize PR and AV relationship
- Holter or event monitor for intermittent block
- Echocardiogram — assess structural heart disease, valvular abnormalities
- Cardiac MRI/PET if infiltrative cardiomyopathy or sarcoidosis suspected
Diagnostic algorithm
| Type | ECG features | Site | Symptoms / risk | Pacing indication |
|---|---|---|---|---|
| First-degree | PR >200 ms, every P conducted | Usually AV node | Asymptomatic | Not indicated |
| Mobitz I (Wenckebach) | Progressive PR lengthening, then dropped QRS | AV node | Usually asymptomatic | Only if symptomatic |
| Mobitz II | Constant PR, sudden dropped QRS | Infranodal (His-Purkinje) | Syncope; high progression risk | Yes — Class I |
| High-grade (2:1 or worse) | ≥2 consecutive blocked P waves | Variable | Bradycardia, syncope | Usually yes |
| Third-degree (complete) | AV dissociation; atrial rate > ventricular escape | Anywhere; usually infranodal | Syncope, sudden death | Yes — Class I |
Treatment
First-line
- Identify and remove reversible causes: hold AV nodal blockers, correct electrolytes, treat ischemia, treat Lyme
- Asymptomatic first-degree and Mobitz I (with narrow QRS): no specific therapy, observation
- Symptomatic bradycardia: atropine 0.5-1 mg IV q3-5 min up to 3 mg total (effective for nodal blocks, less so for infranodal)
- Transcutaneous pacing for unstable symptomatic block as bridge to transvenous pacing
- Dopamine 5-20 mcg/kg/min or epinephrine 2-10 mcg/min as alternatives if atropine fails
Second-line / adjunct
- Permanent pacemaker (Class I) for: symptomatic Mobitz I or Mobitz II, any third-degree AV block (symptomatic or asymptomatic with significant escape pauses), advanced second-degree block
- Permanent pacemaker (Class IIa) for: asymptomatic Mobitz II, asymptomatic high-grade block with average HR <40, alternating bundle branch block
- Dual-chamber pacing preferred over single-chamber for sinus rhythm with intact atrial activity
- Avoid permanent pacing for reversible causes (drug effect, electrolyte, Lyme — most resolve with treatment)
- Cardiac resynchronization therapy if EF ≤35% and significant ventricular pacing burden expected
Complications
- Syncope with injury (Stokes-Adams attack)
- Sudden cardiac death from asystole or ventricular escape failure
- Heart failure from chronic bradycardia and AV dyssynchrony
- Pacemaker complications: lead displacement, infection, RV pacing-induced cardiomyopathy
- Tachy-brady syndrome (sick sinus) — pause-dependent symptoms
PANCE pearls
- Mobitz I (Wenckebach) with NARROW QRS is usually nodal and benign; Mobitz II is infranodal and warrants a pacemaker.
- Atropine is effective for AV nodal blocks but may paradoxically worsen infranodal blocks by speeding atrial rate without improving conduction.
- Inferior MI causes transient AV nodal block (RCA supplies AV node in ~90%) — usually resolves; rarely needs permanent pacing.
- Anterior MI with new AV block reflects extensive infranodal damage and carries high mortality — often needs pacing.
- Always check for reversible causes (drugs, Lyme, electrolytes) before committing a patient to a permanent pacemaker.
Images
References
- ACC/AHA/HRS 2018 Bradycardia — 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay (Kusumoto et al., Circulation 2019)
- ESC 2021 Pacing — 2021 ESC Guidelines on Cardiac Pacing and Cardiac Resynchronization Therapy (Glikson et al., Eur Heart J 2021)
Practice Cardiovascular questions on FirstPassPA
Turn this outline into retention. 5,500+ board-style questions with an AI tutor that explains every answer — free to start, no card required.
Start studying free → Browse all 514 diagnosesEducational use only. This outline is a study aid for PA students and is not medical advice or a substitute for clinical judgment. FirstPassPA is an independent study tool and is not affiliated with, endorsed by, or sponsored by NCCPA or PAEA. PANCE® and PANRE® are registered trademarks of the National Commission on Certification of Physician Assistants; End of Rotation™ is a program of the Physician Assistant Education Association.